Nerve Tension and Scoliosis
Written and reviewed for scientific and factual accuracy by Dr. Austin Jelcick, PhD and Dr. Matthew Janzen, DC. Last reviewed/edited on January 1st, 2026. First published November 6, 2019.
Scoliosis has been treated for centuries, with some of the first treatments being described in the 5th century BC by Hippocrates. Yet despite over 2000 years of history the cause of scoliosis, in particular idiopathic scoliosis has remained an elusive mystery. However, in the 1960’s the idea that a tight or short spinal cord could be the underlying cause of idiopathic scoliosis was described by Dr. Milan Roth. Since then, other doctors and researchers have made observations that match Dr. Roth’s hypothesis, including MRI images that match Dr. Roth’s observations adding more evidence to support his hypothesis. So how exactly do tight nerves (nerve tension) and a tight or short spinal cord cause a scoliosis to develop?
The Spine and Spinal Cord: What’s “Normal”?
Before we talk about nerve tension and how it relates to the development of scoliosis and the rib hump commonly seen in patients with scoliosis, let’s first quickly talk about the normal curvature of the spine. A normal healthy spine will naturally have some curvature in various locations that help to distribute the force/load of the effects of gravity. After all, and adult head weights about 10-11 pounds. If you look at the image to the right (below if you are on mobile) you can see a breakdown of these curves.
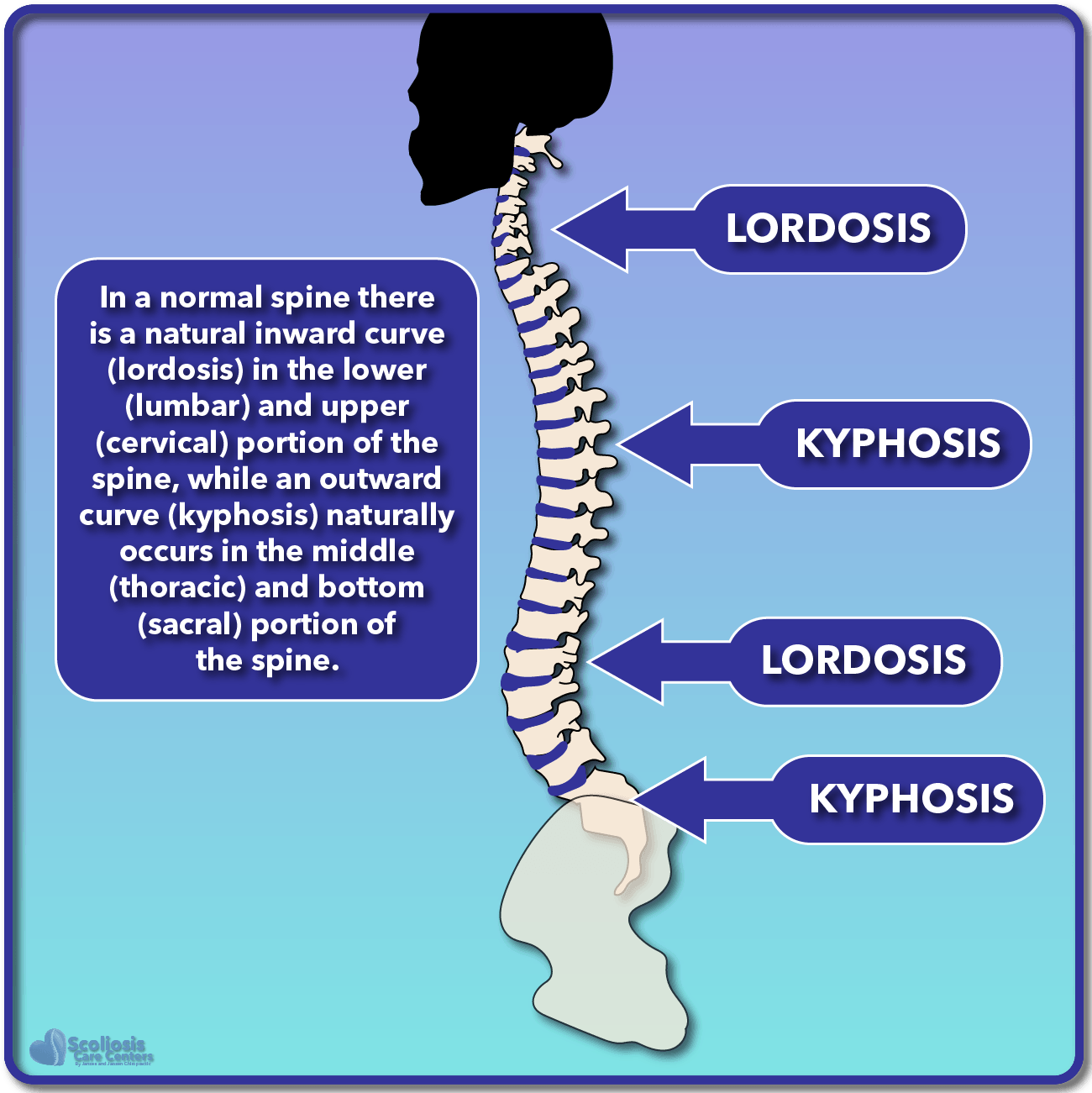
In our example the spine (and body) are facing to the left; thus any “inward” curve would be curving to the left, while any “outward” curve is going to the right.
The inward curve is commonly referred to as lordosis, and natural occurs in the cervical and lumbar portions of the spine. The outward curve is commonly known as kyphosis (not to be confused with hyperkyphosis) and naturally occurs in the thoracic and sacral portions of the spine. Understanding the normal curves present in the spine is helpful as we begin to talk about how the spine will twist (rotate) and collapse when nerve tension is present.
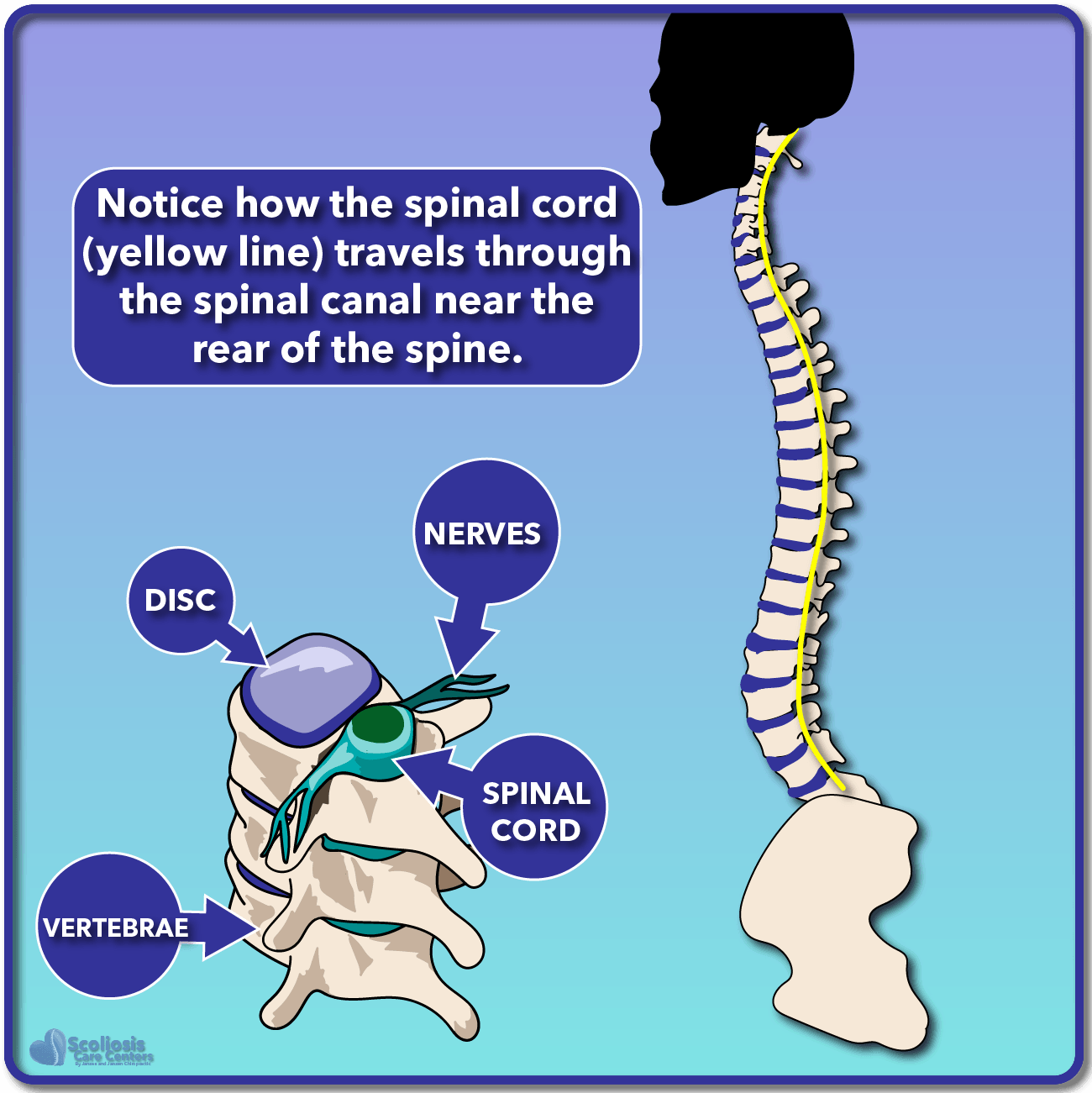
If we once again look at our normal healthy spine, we can also see where the spinal cord normally travels. As shown in the illustrated cross-section, you can see the vertebrae, disc, nerves, and spinal cord. While it might seem like the spinal cord goes right down the middle of the spine, it actually is located towards the rear of the spine, running down the length of the spinal canal. The spinal cord will attempt to take the shortest path possible (the path of least resistance) as it runs down the spinal canal, which can mean it isn’t always right down the center of the spinal canal. We’ll talk about this again in a minute.
Nerve Tension: How Does It Affect The Spine?
A scientist by the name of Dr. Roth developed the concept that if the nerves (spinal cord included) grew slower than the spine, there could be essentially a “mismatch” where the spine was now longer than the nerves, the spinal cord and nerves would be pulled tight in an attempt to “keep up” with the spine 1, 2. If the imbalance became too severe, the spine would rotate and collapse to provide the spinal cord and nerves with the shortest path possible. But why would it rotate and collapse?
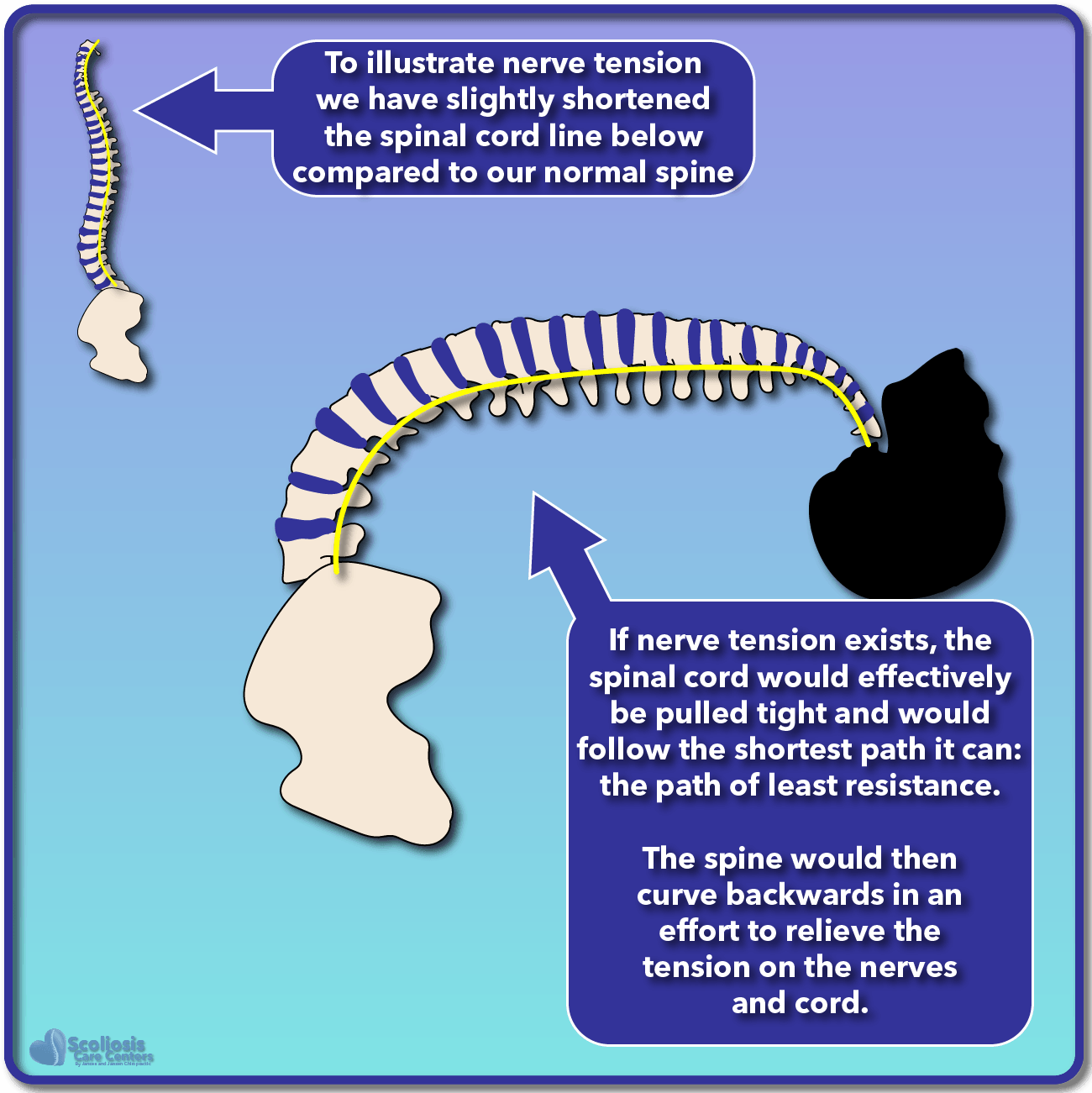
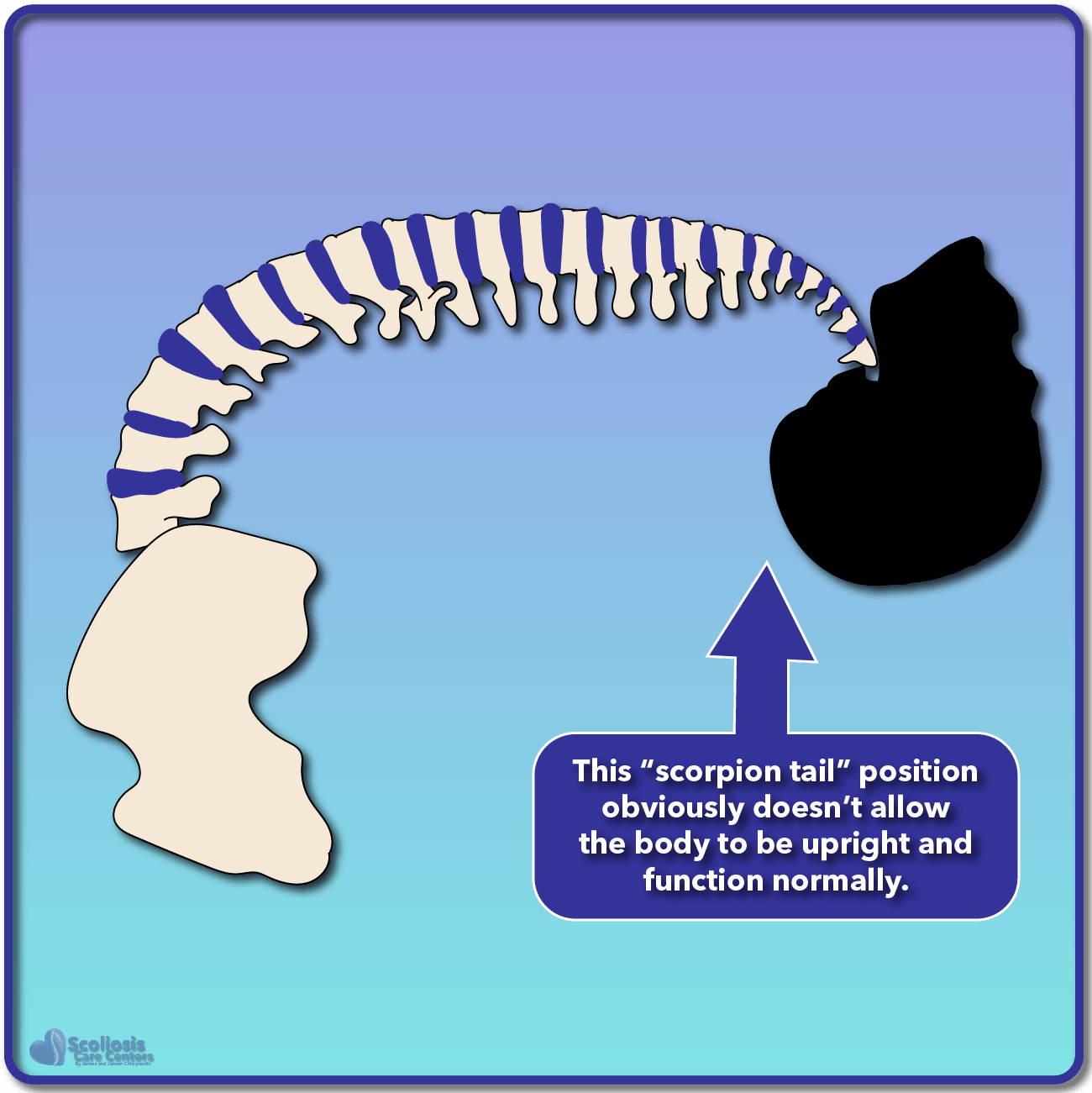
If we look at these illustrations we can see the “normal” spine with the spinal cord traveling down the length of the spine. In the case of nerve tension, our spinal cord would be slightly shorter, and as a result the increased tension would cause the spine to curve back like a scorpion’s tail as shown. This scorpion posture would relieve the tension on the nerves and cord, but obviously doesn’t work well for walking around, and we don’t see people walking around with their backs arched and their heads facing towards the sky. This is where our natural “righting reflex” comes in that allows the head and eyes to face forward.
Something’s Gotta Give: How The Spine Tries to Relieve Nerve Tension
Since our spinal cord and nerves are tight, the spine is pulled back into a scorpion position; but this doesn’t allow us to walk upright or look in front of us. The natural righting reflex puts out head upright once more, but we no longer have that short path for the spinal cord to follow. We now need a new path of least resistance.
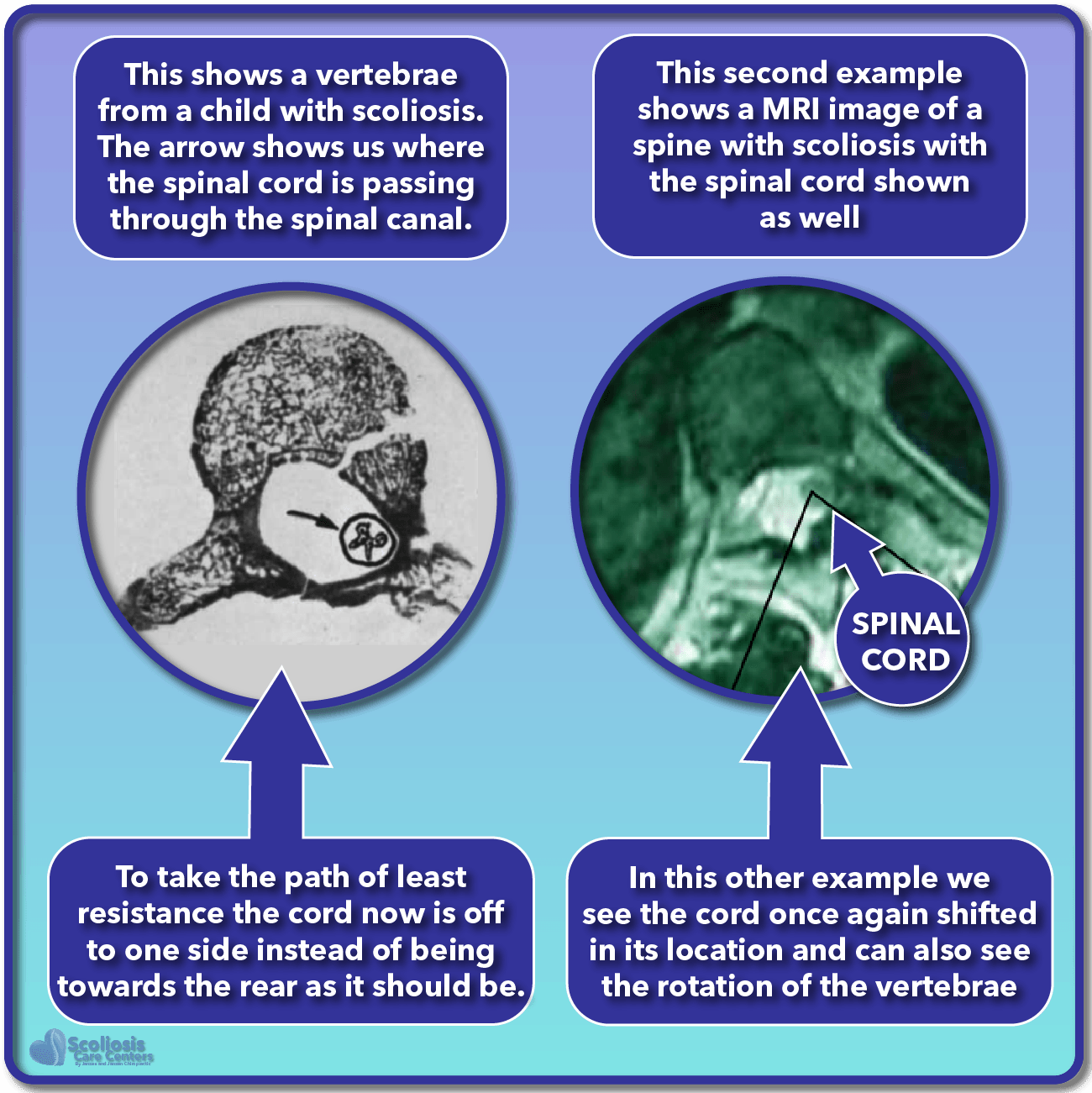
To provide the tight nerves with the shortest path possible, the spine rotates and collapses into the posture and shape we typically see with scoliosis. If you remember from the cross section illustration above, the spinal cord travels down the spinal canal which is near the rear of the spine. Because of the need to find the shortest path possible, the spinal cord can also shift within the spinal canal, residing more on one side than the other depending on the direction of rotation and the scoliosis curve.

In the example shown, we see two images: one of an xray of a vertebrae from a six and a half year old child who had a scoliosis curve which curved to the right and one of a MRI of the spine showing the vertebrae and spinal cord in a 38 year old patient 4 with untreated scoliosis. We can see a cross section of where the spinal cord was running through the spinal canal. In order to follow the shortest path possible, the spinal cord has shifted off to one side of the spinal canal. In these examples, the scoliosis curve is opposite from the side the cord shifts to. A better way to describe this is that the convex side of the curve is opposite from the side the cord shifted towards (the concave side). Let’s look at the spine from the front to get a better understanding of what’s going on.
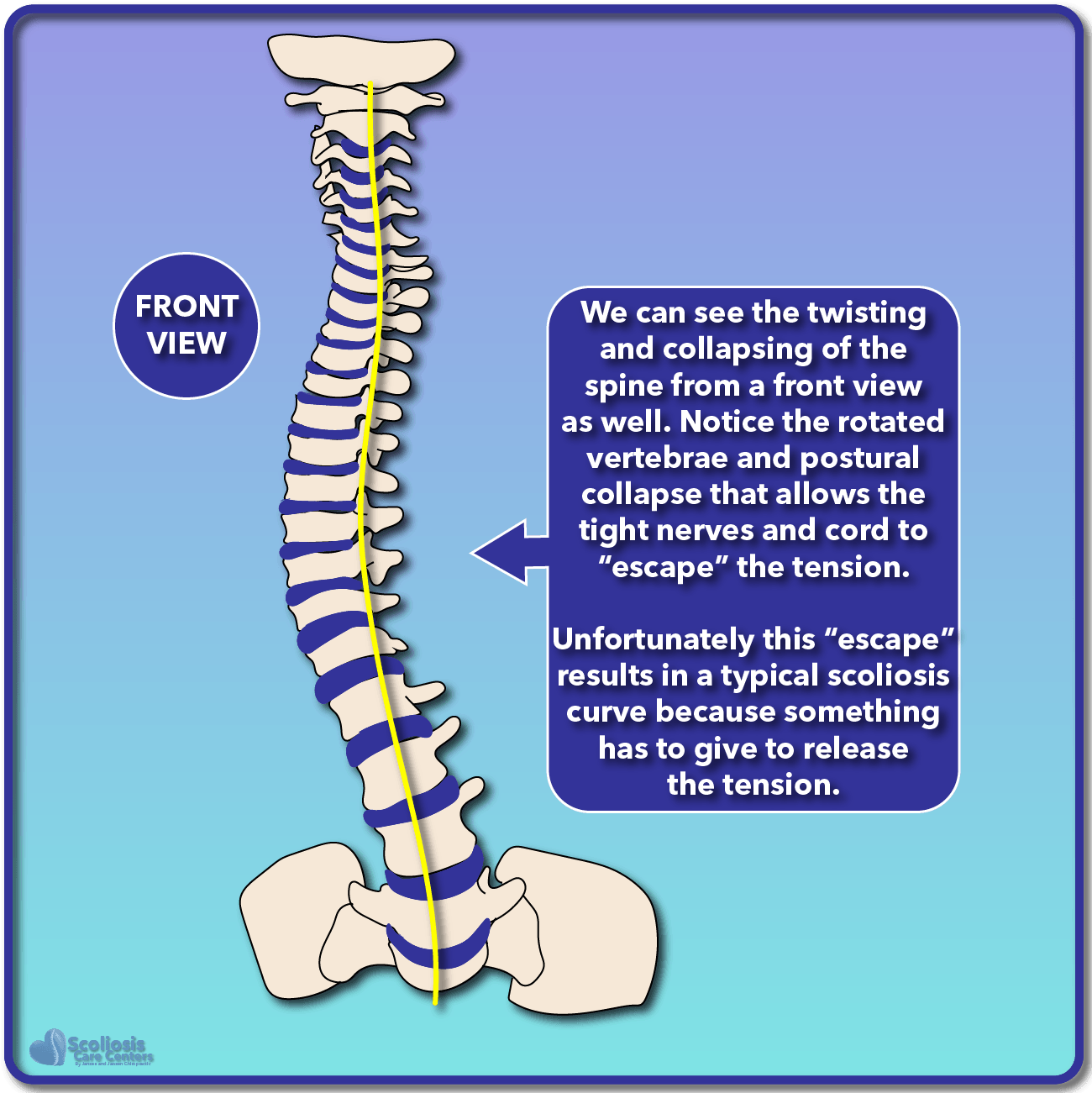
In the example shown to the right (below on mobile) we see the spine viewed from the front, with the base of the skull shown at the top and the top of the pelvis shown at the bottom. The spinal cord is once again illustrated as a yellow line which attempts to take the shortest path possible down the spinal canal. Because the spinal canal is at the rear of each vertebrae, the spine rotates and collapses to provide the shortest path possible. This also better shows show the spinal cord can shift to one side. This illustration is the opposite of our vertebrae xray: the scoliosis curve goes to the left (convex side of the curve) while our spinal cord shifts to the right (concave side of the curve).
Tying It All Together: Nerve Tension, Scoliosis, and Rib Hump
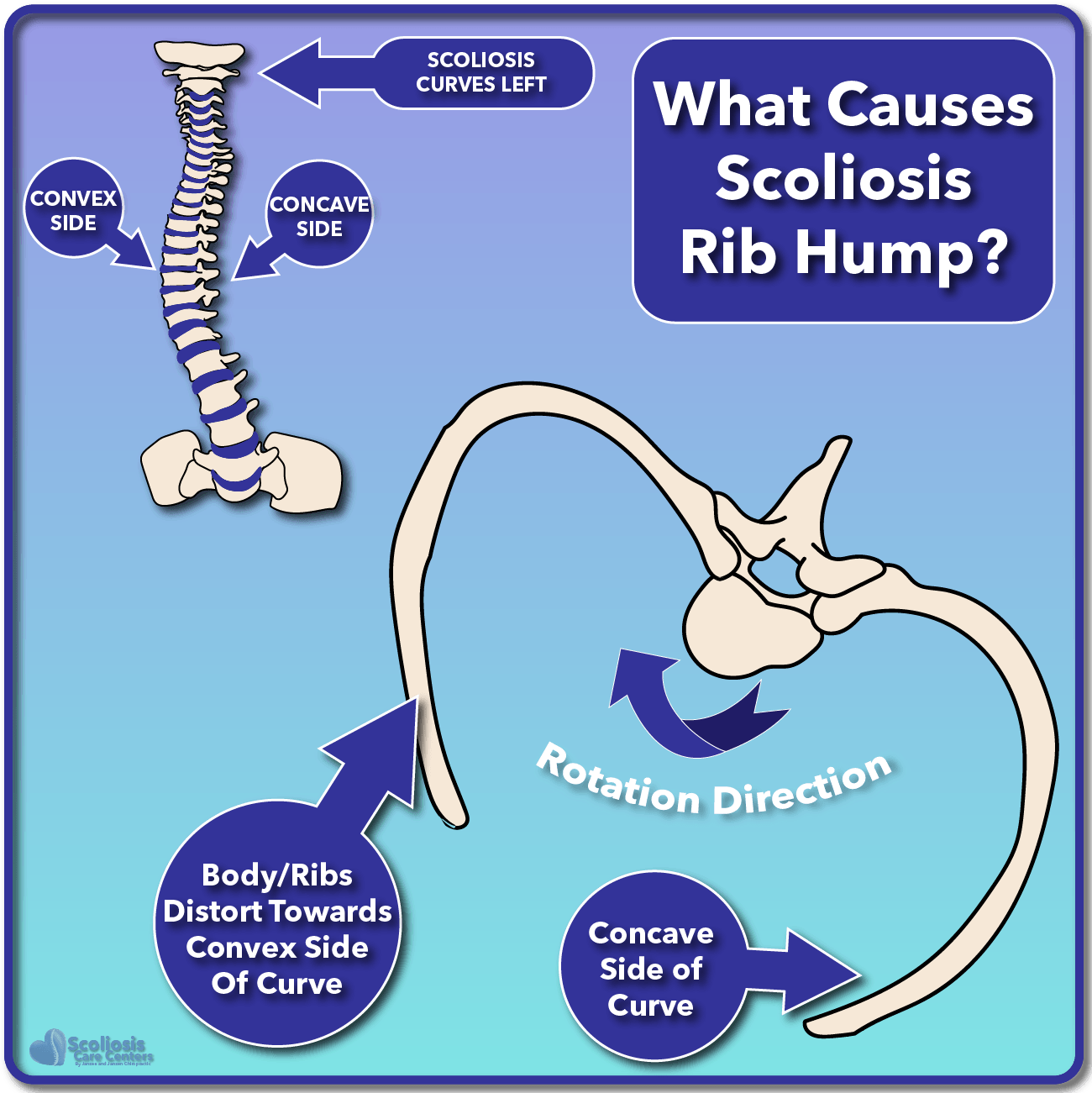
If we look at everything together, we now see a complete picture where rib hump is both related to scoliosis and nerve tension. As illustrated to the right (below on mobile) we can see how the ribs become distorted and a rib hump forms as a result of the rotation of the spine. As the spine rotates, the body and ribs distort towards the convex side of the scoliosis curve, causing a rib hump to form on that side. Meanwhile, the ribs on the concave side distort the opposite direction, giving us the classical rib hump we see when a scoliosis curve is present. In fact when scoliosis is treated with surgery (using screws and rods), it was found that causing rotation from tightening the rods too much caused an increased rib hump as a result 3.
However, it can be quite common when screening for scoliosis to see a rib hump, but a scoliosis isn’t easily visible. This is known as a “false positive” because the result of our screening test (the forward bending Adam’s test) shows a rib hump which should indicate a scoliosis exists, yet for some reason we don’t see a scoliosis curve. The missing piece of the puzzle then is nerve tension.
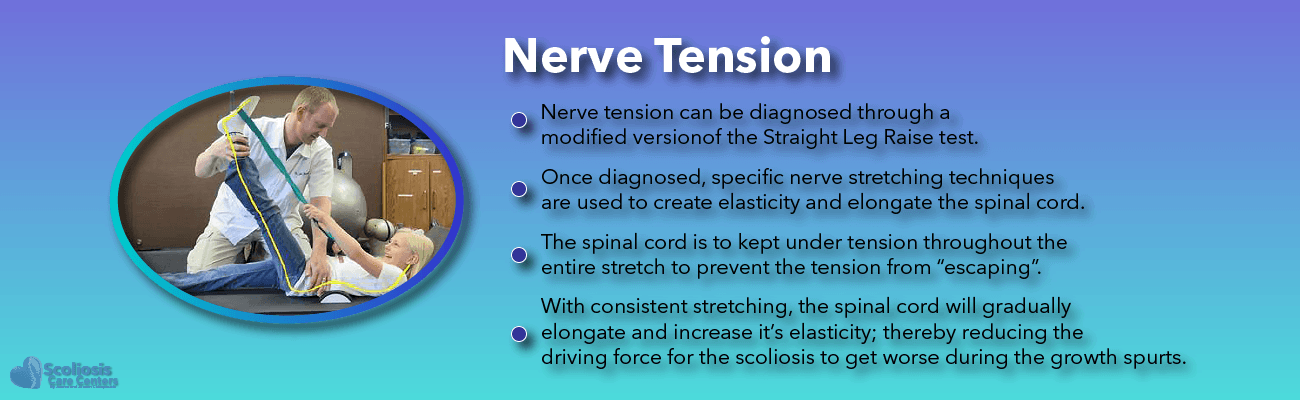
Based on Dr. Roth’s nerve tension hypothesis, it would appear that the Adam’s forward bending test, while used for detecting a scoliosis curve, may actually have another helpful use: a nerve tension test. If we look at the spine and rib cage during a normal Adam’s test, we see the spine bending forward, and the ribs looking more or less symmetric as well. But what happens if nerve tension is present?
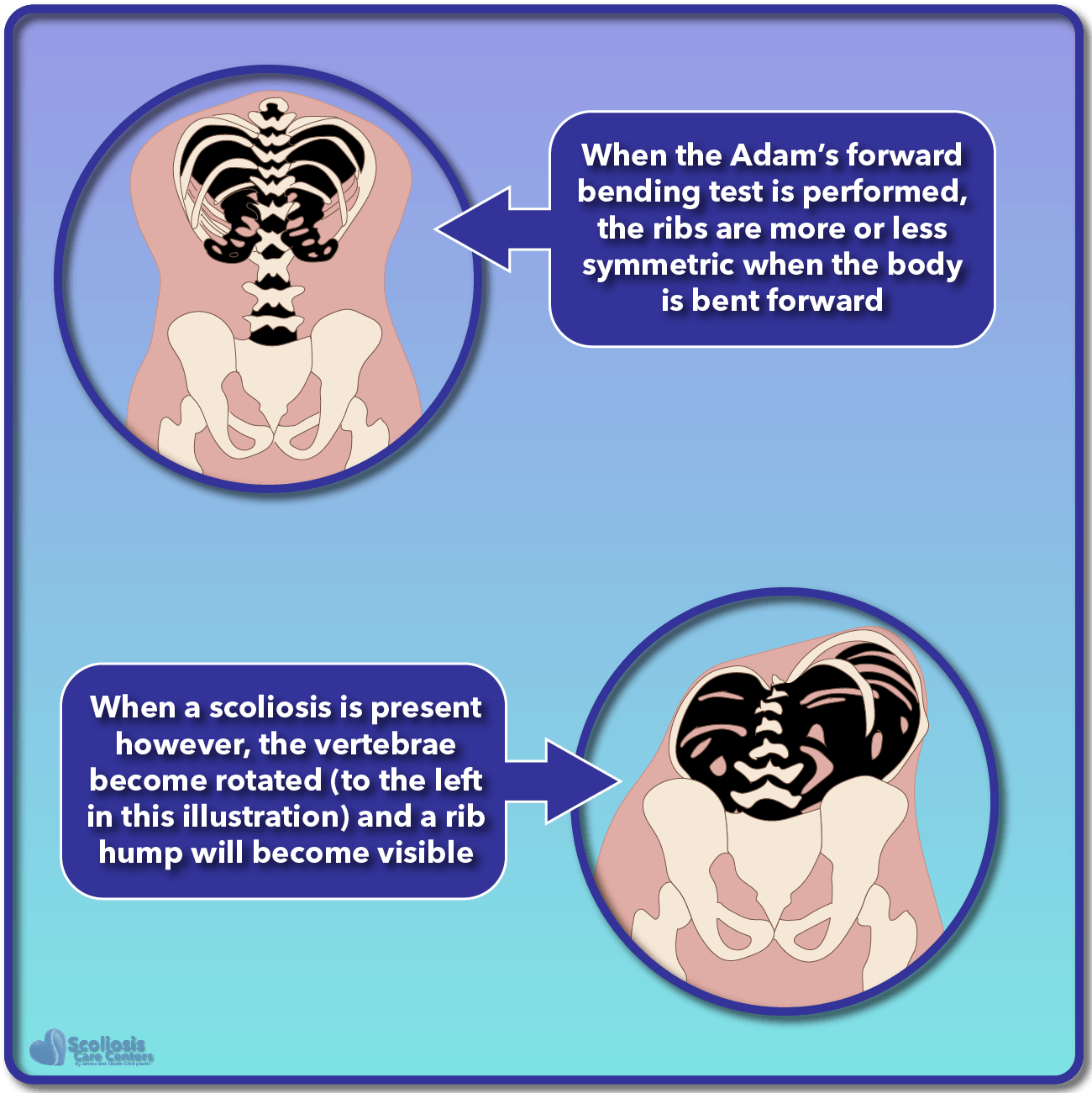
As we talked about earlier, a scoliosis can develop as a result of nerve tension when the spine grows faster than the spinal cord and nerves. However, if growth hasn’t sped up yet (think growth spurts) the spine may not need to rotate and collapse to accommodate the tight nerves YET. Instead, we simply have increased tension when we flex the spine and attempt to stretch the tight nerves and cord. The result is that when we bend over, the spine will rotate to try and accommodate our tight nerves and because of this rotation, we see a subtle rib hump.
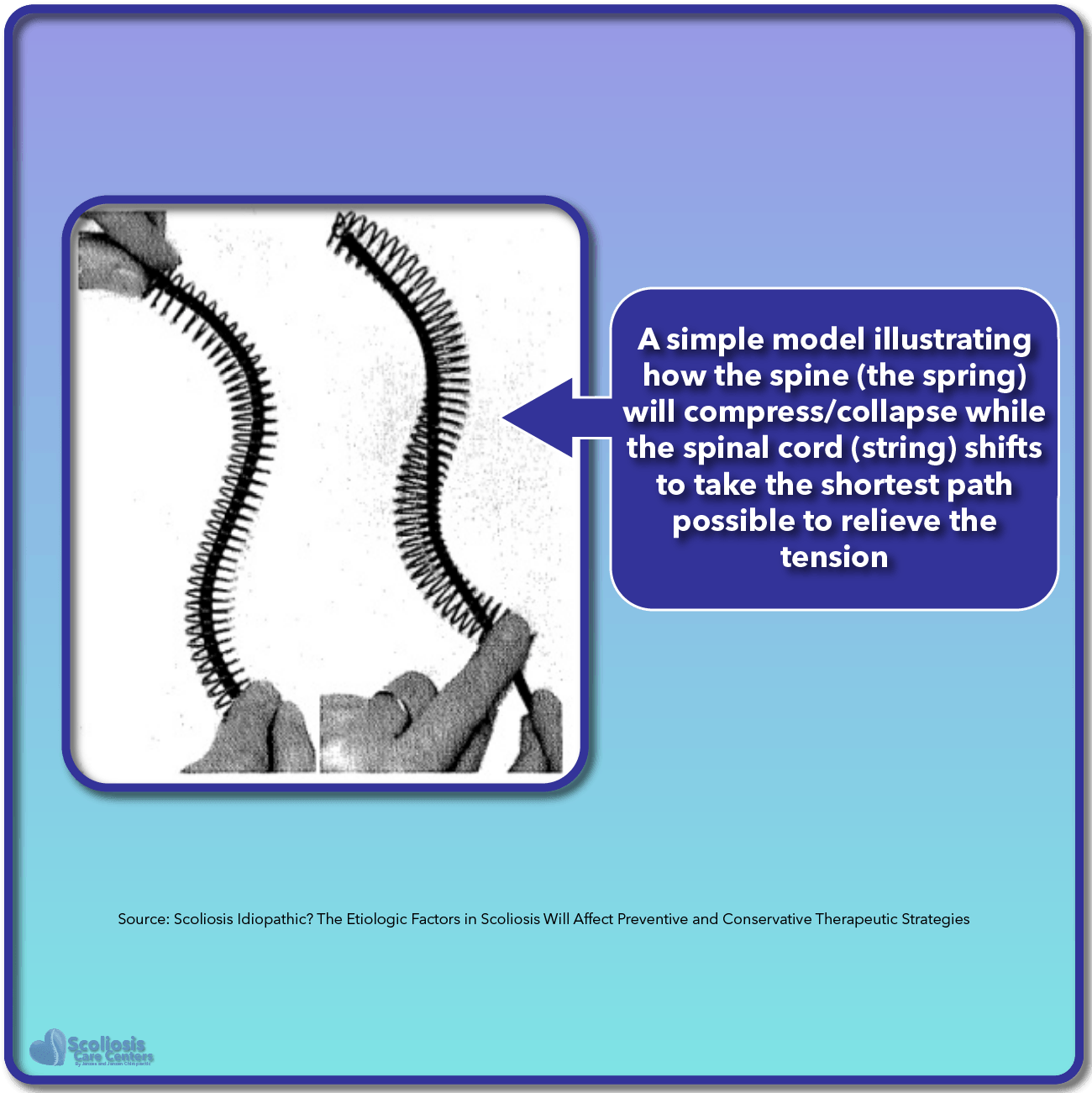
Dr. Roth provided an eloquent model of just how nerve tension can affect the spine and cause the rotation and collapse seen in scoliosis by using a spring and a string. By pulling the string tight to simulate nerve tension or a short spinal cord, we see the spring (the spine) collapse and the string (the cord) shift in its location so that it takes the shortest path possible. This model is similar to what we see in scoliosis and provides a simpler more intuitive illustration of how the spine collapses to accommodate the tight/short cord.
The Adam’s Forward Bending Test: Now For Detecting Nerve Tension?
The subtle rib hump that exists as a result of tight nerves is an important observation. In this case the spine and nerves have not yet become so disproportionately different in length that the rotation and collapse of the spine has not yet occurred, and so we do not observe a scoliosis. Yet our Adam’s test suggests a scoliosis exists but is essentially a false positive for scoliosis. But in reality it isn’t a false positive result for scoliosis, but instead a positive test for nerve tension. Nerve tension can also be detected using a clinical test 4 known as a Cox test.
Because of the nerve tension that exists, a scoliosis can develop once the body reaches a period of rapid growth (growth spurt) and the growth of the spine takes off while leaving the spinal cord and nerves in the dust. However if we can detect tight nerves BEFORE the scoliosis has a chance to develop, we can treat both the tight nerves and the potential scoliosis and prevent a problem before it occurs.
A Recipe For Success: Treating Nerve Tension and Scoliosis
A neurosurgeon by the name of Dr. Breig was one of the first people to observe how much the spinal cord stretched or elongated and found that during flexion (ie stretching) it would elongate by about 5-7 cm 5. Thus if we can stretch the tight nerves, and gradually stretch and lengthen the spinal cord we can reduce nerve tension and the driving force behind scoliosis. If the tight nerves are addressed, the spine doesn’t need to rotate and collapse as much to accommodate the tight nerves.
Since the spine can grow faster than the nerves/spinal cord during growth spurts, we also need a way to hold the spine straight so it is not allowed to rotate and collapse. What we need is a brace to hold the spine straight while it grows. If we do this, while also treating the underlying nerve tension, we effectively treat all aspects of the scoliosis, the nerve tension, and thus the rib hump as well. The final result is a proactive treatment and prevention for scoliosis that reduces or eliminates rib hump, while allowing the spine to grow as straight as possible, and is now permanently straighter after reaching skeletal maturity.
References
- Roth, M. (1981): Idiopathic scoliosis from the point of view of the neuroradiologist. In Neuroradiology 21 (3), pp. 133–138.
- Roth, M. (1968): Idiopathic scoliosis caused by a short spinal cord. In Acta radiologica: diagnosis 7 (3), pp. 257–271.
- Pizones, Javier; Sánchez-Mariscal, Felisa; Zúñiga, Lorenzo; Izquierdo, Enrique (2016): The effect of sublaminar wires on the rib hump deformity during scoliosis correction manoeuvres. In European journal of orthopaedic surgery & traumatology : orthopedie traumatologie 26 (7), pp. 771–777.
- Van Loon, Piet J.M. (2012): Scoliosis Idiopathic? The Etiologic Factors in Scoliosis Will Affect Preventive and Conservative Therapeutic Strategies: IntechOpen, 5/9/2012.
- Breig, A. (1979): Adverse mechanical tension in the central nervous system, by Alf Brieg, Almquist & Wiksell, Stockholm, 1978, 264 pp, illustrated. In Annals of neurology 6 (5), p. 460.