Release Contractures That Cause Stiffness
Scoliosis Flexibility Trainer
Written and reviewed for scientific and factual accuracy by Dr. Austin Jelcick, PhD and Dr. Matthew Janzen, DC. Last reviewed/edited on October 27, 2020.

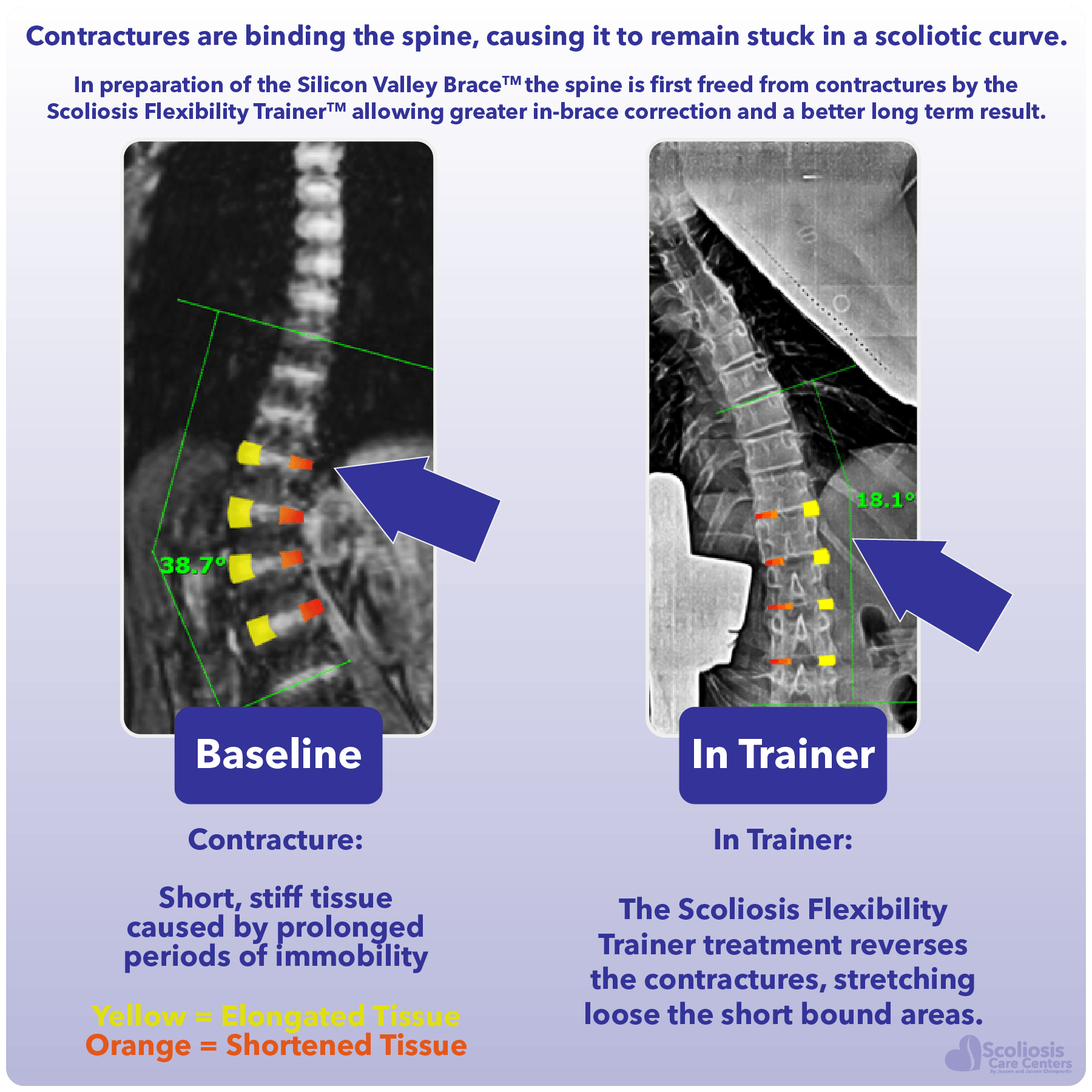
The Scoliosis Flexibility Trainer is a unique FDA registered device that helps to unbend and untwist a scoliosis curve non-surgically, providing drastically better non-surgical treatment results. It accomplishes this feat by addressing a problem that every surgeon knows about and has to deal with, yet most (if not all) non-surgical approaches ignore: the problem of contractures.
But how does it work, and why does it work so well at straightening and untwisting the spine? What problems does it solve that other non-surgical treatments don’t? Let’s first look at the contracture problem that is ignored by most non-surgical approaches, yet addressed by every surgeon who performs surgery for scoliosis.

While we discuss contractures in a minute, what you need to know is that contractures make the spine “stiff” and limit how straight it can be made with treatment. You also need to know that surgeons “release” contractures the only way they know how: by cutting them out.
While this may “release” the contractures it also permanently destroys the joint and tissue. This requires the surgeon to fuse those sections of the spine which in turn permanently reduces mobility/range of motion. This process is not something that happens occasionally but is actually ROUTINE as releasing contractures/stiffness is a standard operative procedure for scoliosis.
The Scoliosis Flexibility Trainer avoids the destruction of these important spinal joints completely by providing an effective non-surgical way to release contractures. This increases range of motion of the spine, reduces the scoliosis curve, and prepares the spine to be better straightened in brace. All of this works together to provide a drastically better treatment outcome while avoiding the pitfalls and limitations of surgery.
What is a contracture?
Contracture: a stiffening of connective tissue caused by immobilization or reduced range of motion
If you’ve never heard the term contracture before, especially as it relates to scoliosis, you’re not alone. However you may have heard the term contracture before with regards to other joints such as the knee or elbow. “Contracture” is the medical term for changes or stiffening of connective tissues such as ligaments, tendons, and muscles that result in the loss of motion of a joint. A common cause of contractures in joints like the elbow and knee are when the joint is immobilized (such as when wearing a cast) after breaking a bone. Treating contractures through stretching (physical therapy) is routine once the cast comes off so that range of motion is restored. However, what happens when contractures form in the spine?
Contractures and Scoliosis
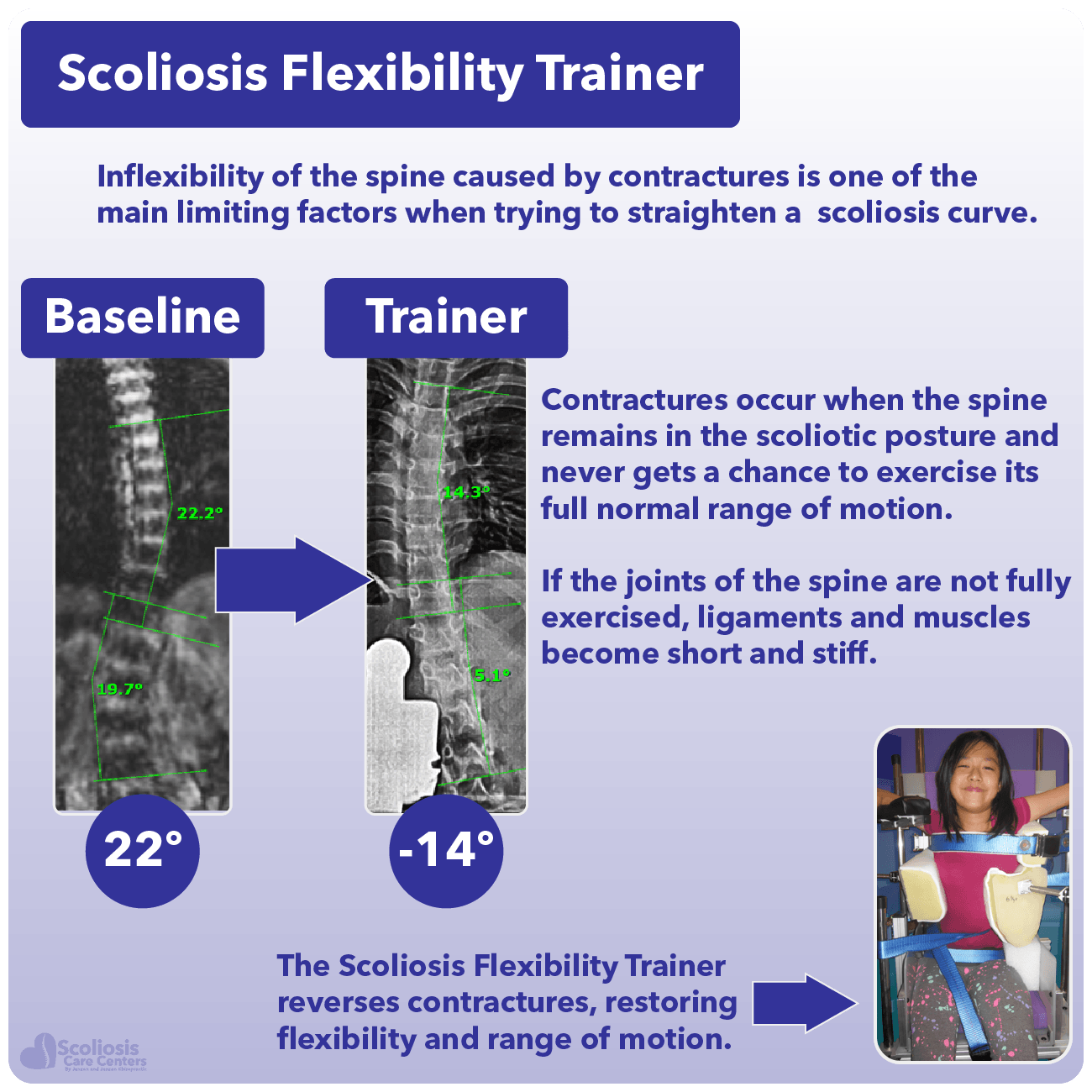
While the elbow and knee are single joints, a typical scoliotic spine may have over 50 different joints affected by contractures. Inflexibility of the spine (stiffness) caused by contractures, is one of the main limiting factors when trying to straighten a curve. Contractures occur when the spine remains in the scoliotic posture and never gets a chance to exercise its full normal range of motion. If the joints of the spine are not fully exercised, the ligaments and muscles become short and stiff. Muscles, ligaments, and discs become shorter on the short concave side of the scoliosis and grow longer on the long convex side.
Contractures and rotation limit how much a spine with scoliosis can be straightened
Pre-operative X-rays
When a person is scheduled for surgery for their scoliosis curve, before they ever lie down on the operating table the surgeon will perform several pre-operative x-rays to assess the curve and the spine as a whole. The surgeon will order several x-rays to be taken of the spine, but with the patient lying down on their back (this is referred to as supine) and then bending from side to side 1. These side bending x-rays are commonly known as “lateral bending x-rays” and their purpose is to determine how rigid or stiff the spine is 2.
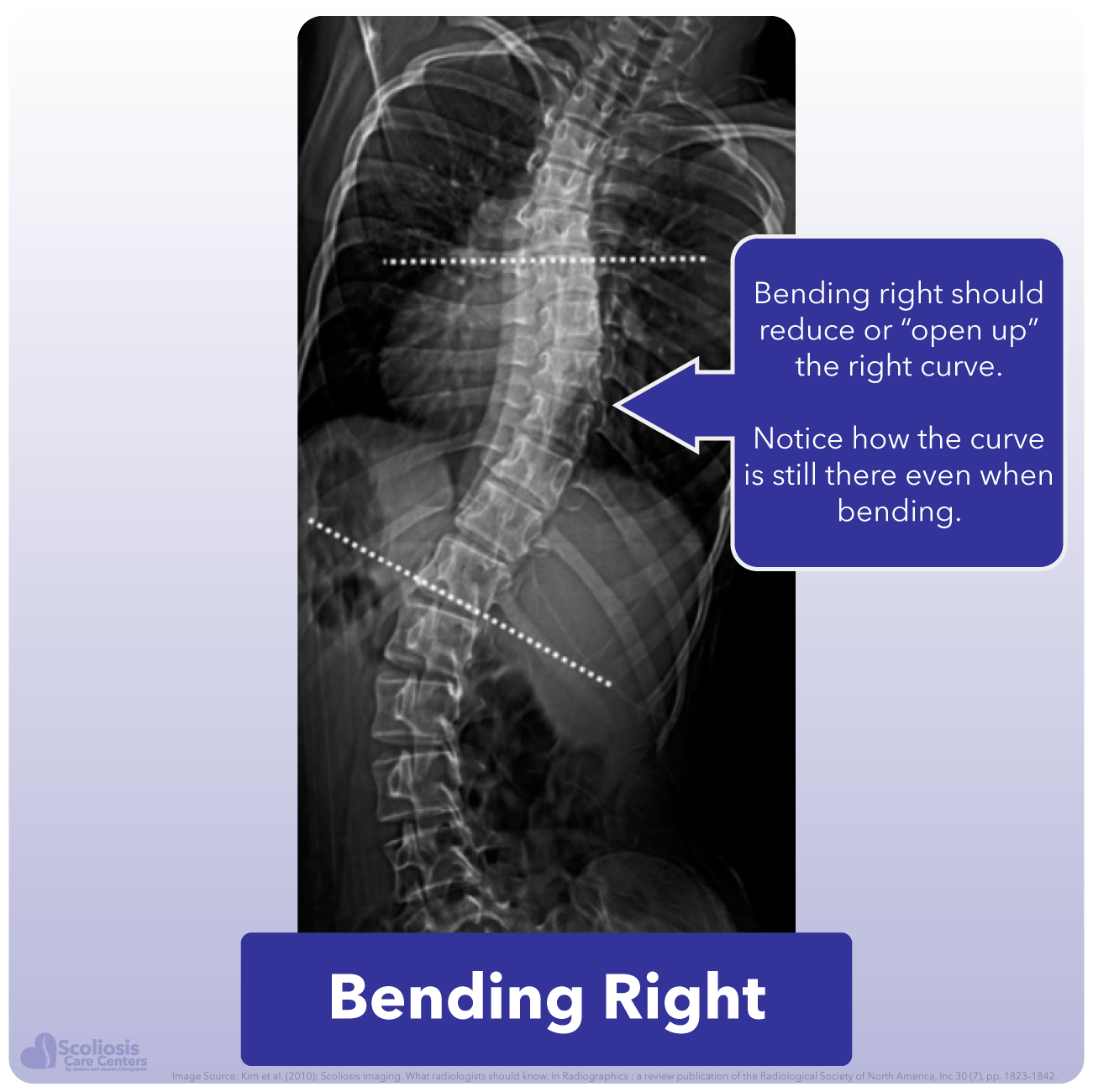
Bending x-rays are taken before surgery to determine how “stiff” the spine/curve are
If we look at these side bending x-rays (example taken from the video above), we can see that even though the patient is bending so that their curve should reduce, the curve persists and does not significantly reduce in size as we might expect. Similarly when the patient bends to the other side, we see the curve get worse. Surgeons will call this a “structural” curve because it persists instead of reducing while bending. However, while truly structural changes in the bone may be present (such as wedging of vertebrae), the curve can be better thought of as “stiff” rather than “structural” because its range of motion is limited by stiff contractured soft tissue and rotation rather than a structural bone change.
When the x-rays indicate that a part of the spine has a “structural” curve that persists despite the side bending, it lets the surgeon know that there are contractures and changes present which need to be addressed. Surgeons commonly refer to the surgical treatment of contractures and “stiffness” as “release”; “surgical release” or “releasing contractures”. Unfortunately during surgery this means that those contractures must be cut out and those inflexible portions of the spine are fused, permanently reducing their range of motion.
This is done on purpose by the surgeon because if they cut out the connective tissue binding the spine and also fuse those sections, they effectively prevent ANY movement in those joints. This prevents the curve from worsening in those regions, but at the cost of eliminating range of motion in those joints/parts of the spine. While the surgical release of contractures is not covered in the video, you can learn how surgeons perform “release” in our educational blog.
Filling the Gap: Releasing Contractures Without Surgery
Checking for contractures is routine before surgery, yet this has been completely ignored when treating scoliosis non-surgically… until now. Realizing that no one was treating contractures in non-surgical care, our clinic designed an FDA registered device with one purpose: to target the same contractures that a surgeon normally cuts out. This non-surgical device device utilizes a targeted sustained stretch that addresses both the bend and the twist of a curve in three-dimensions for each and every segment of the spine involved in the scoliosis curve. However, designing the Scoliosis Flexibility Trainer to accomplish this goal was not without its challenges.
Contractures can be effectively treated without surgery through prolonged targeted stretching
Incomplete Solutions
When you search online for non-surgical treatments for scoliosis you will discover countless videos that show exercises that supposedly help fix a curve. Videos will show someone with a scoliosis performing various bending exercises and claim that this is “opening up” the curve and reducing it. While at first this seems to make sense and a viable (and easy) exercise to perform to help a curve, in reality it is actually doing more harm than good.
Take our example from earlier. The scoliosis curves to the right, so our internet exercise videos would instruct us to bend to open up the curve and reduce it, while also stretching those contractures which exist in the joints of the spine. However, look what happens when we do this: while the main (primary) curve has reduced with our stretch as expected, we have now caused the second curve to get worse. Even worse, these compensatory curves (sometimes called minor curves) can become permanent over time 3 as changes occur in the bone, muscles atrophy, and new contractures form due to a lack of movement/range of motion.
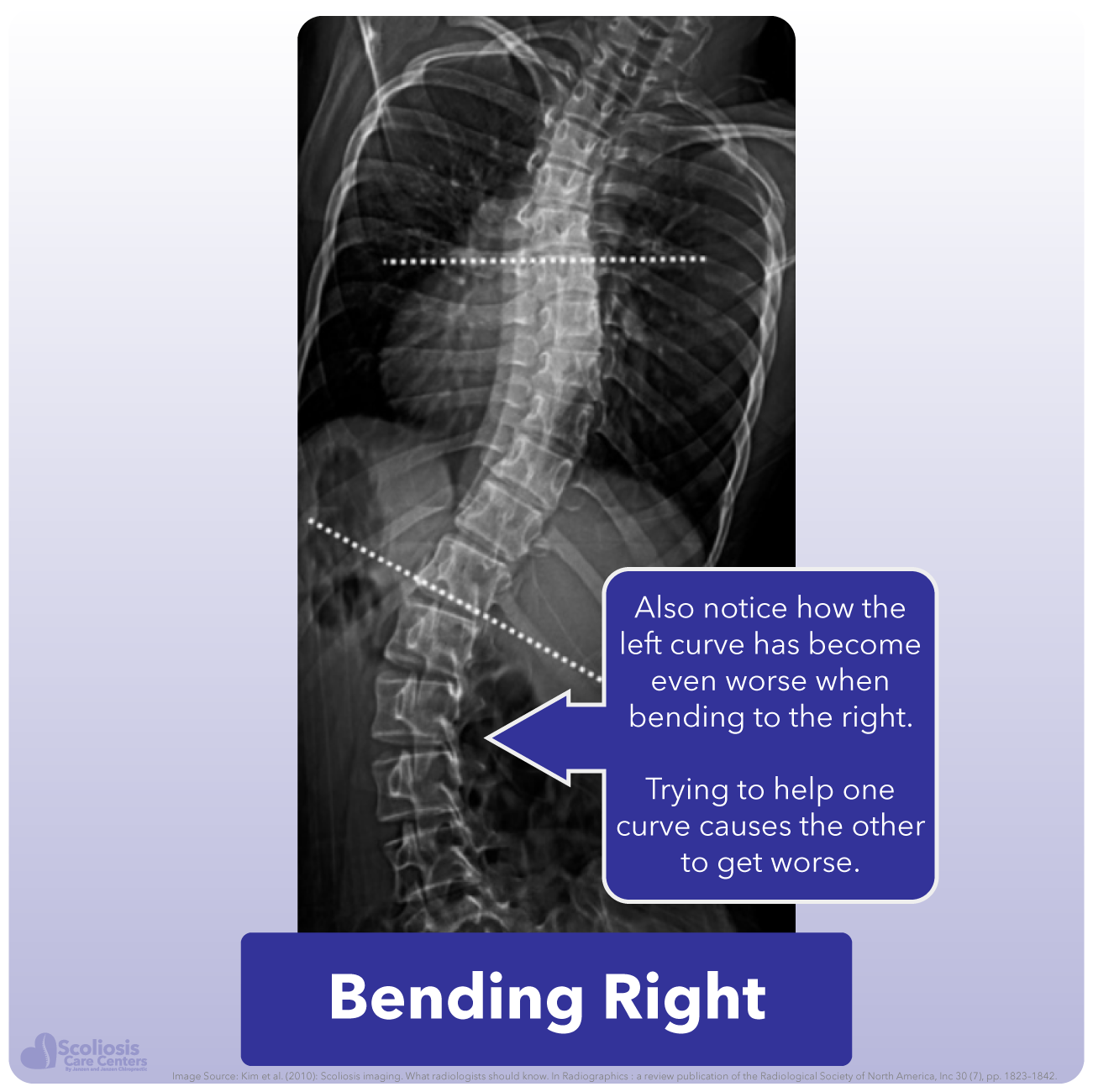
This becomes an even bigger problem for people with S-curves as doing exercises to stretch and reduce one curve will make the other worse, as shown in the example above. This Catch 22 situation we find ourselves in is something every child with a “structural” scoliosis has to deal with, and something surgeons are well aware of. This is why surgeons will repeatedly tell patients that exercises won’t help because of this vicious cycle where any exercise or movement will tend to make the spine worse in one way or another.
The scoliosis Catch 22: Trying to reduce one curve often results in a second curve worsening
Breaking the vicious cycle with the Scoliosis Flexibility Trainer
Preventing these compensatory curves while stretching the contractures of the primary curve effectively breaks this Catch 22 cycle. This then allows effective non-surgical release of contractures while increasing the range of motion of the spine, and is EXACTLY what the Scoliosis Flexibility Trainer is designed to do. Providing device assisted stretching which utilizes multiple contact points on the spine, the Scoliosis Flexibility Trainer supports each and every part of the scoliosis curve while allowing each curve to be INDIVIDUALLY hyper-corrected.
This hypercorrection is a BIG DEAL because not only does it increase the range of motion that was lost due to the curve being “stuck” for a long period of time, but it also stretches those shortened contractured tissues. This non-surgical release of contractures now allows the spine to be moved into a much more straight position, drastically increasing how straight the spine is in the brace thereby improving how much the curve is reduced and treatment outcome.
The Scoliosis Flexibility Trainer effectively hyper-corrects each curve and treats contractures restoring range of motion to the spine
Examples of the Scoliosis Flexibility Trainer in Action
In each example shown in the video above, we can see images of the spine before and during use of the Scoliosis Flexibility Trainer. While the amount of motion restored varies from patient to patient, you can see just how much the spine and its joints are stretched while using the device. Just as a physical therapist will hold a stretch for the knee or elbow, the Scoliosis Flexibility Trainer allows each joint in the spine to be held in a stretched position, releasing contractures non-surgically.
With contractures now addressed, and with our nerve tension being addressed as well, we are ready to use a hyper-corrective brace to hold the spine in a straighter position and allow it to grow straighter permanently. You can learn more about how we use our own hyper-corrective brace, the Silicon Valley Brace, as well as physiotherapeutic scoliosis-specific exercises that accompany wearing the brace in the next sections.Back: Treating the cause of scoliosisNext: Bracing reinvented with the Silicon Valley Brace
References
- Bekki, H. et al. Which Side-Bending X-ray Position is Better to Evaluate the Preoperative Curve Flexibility in Adolescent Idiopathic Scoliosis Patients, Supine or Prone? Asian spine journal 12, 632–638; 10.31616/asj.2018.12.4.632 (2018).
- Kim, H. et al. Scoliosis imaging. What radiologists should know. Radiographics : a review publication of the Radiological Society of North America, Inc 30, 1823–1842; 10.1148/rg.307105061 (2010).
- Malfair, D. et al. Radiographic evaluation of scoliosis. Review. AJR. American journal of roentgenology