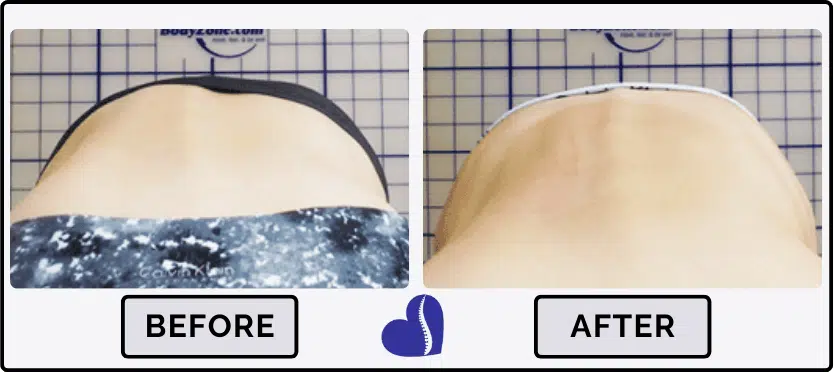
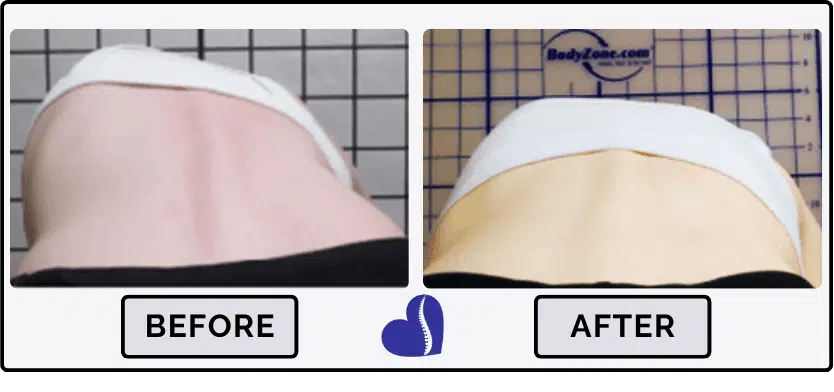
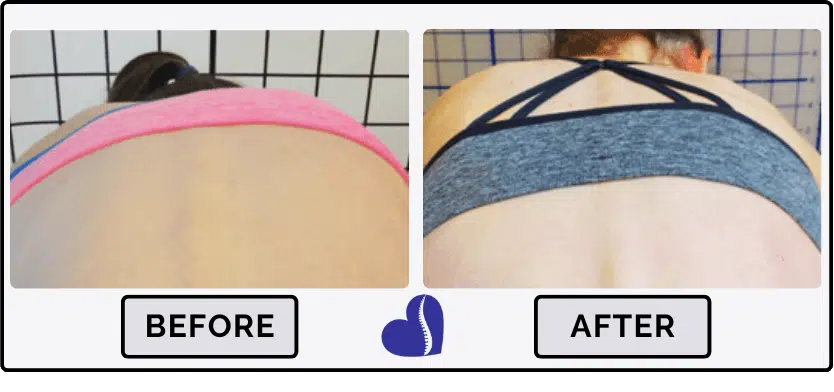
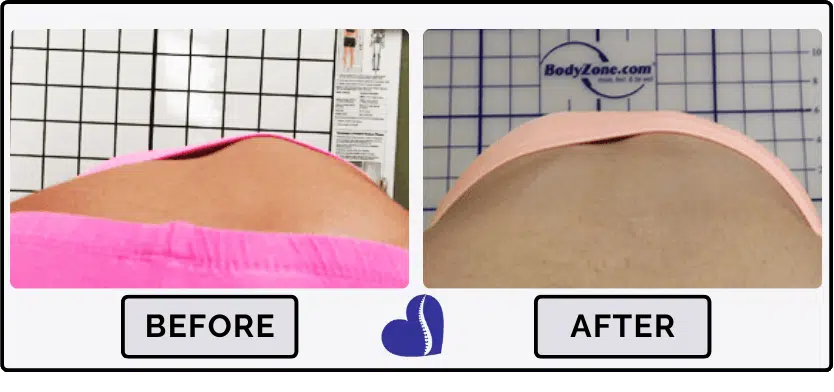
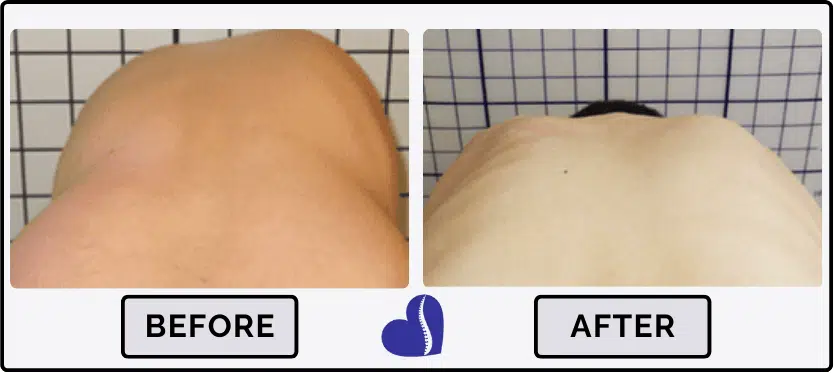
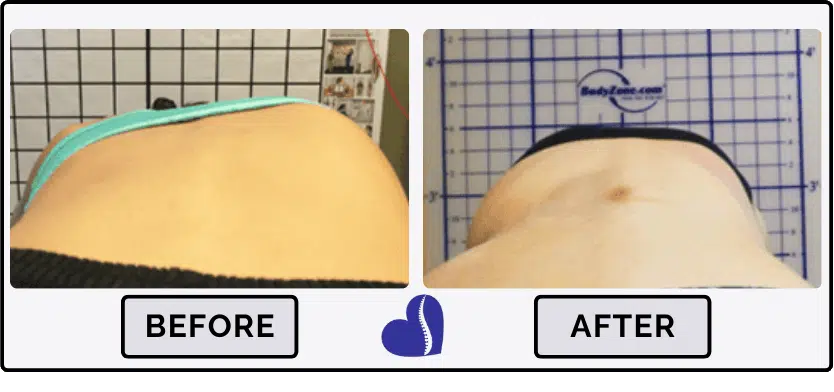
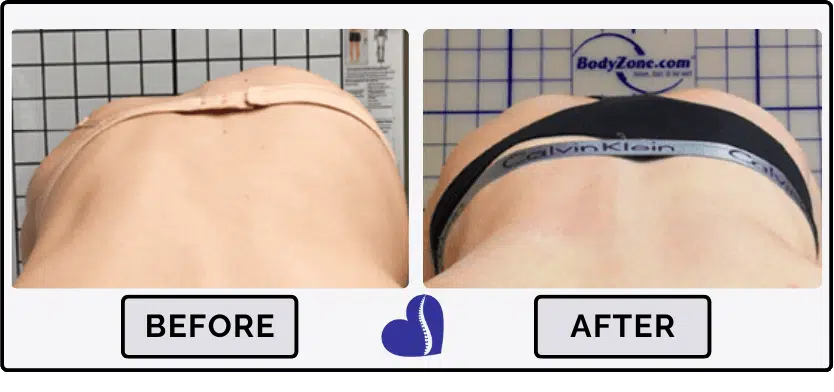
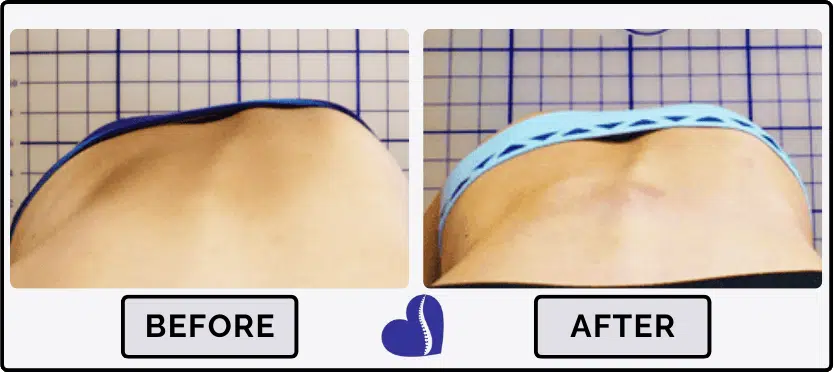
Scoliosis Treatment Results by Rib Hump Improvements
A rib hump is a key indicator of scoliosis as well as the progression of scoliosis when observed in adolescents. A rib hump is identified during the Adam’s forward bending test. If there is asymmetry in the rib height or there is a noticeable curve in the spine it is very likely that the spine has scoliosis. Just as a rib hump is a key indicator of scoliosis, the regression of a rib hump is an indicator of effective scoliosis treatment and curve reduction.


See How We Can Improve Your Child’s Rib Hump – Contact Us Today!
What causes a rib hump?
A rib hump can be one of the most visible signs of scoliosis, but what exactly causes a rib hump? You may have observed that the SIZE of the rib hump can appear to be related to the SEVERITY of the scoliosis (the size of the curve). But if we look closely at the rib cage and the spine, we begin to see that the size of the scoliosis curve isn’t the real culprit. Instead, it would seem that the amount of rotation (remember, scoliosis is a 3-dimensional condition) is more directly related to the size of the rib hump. So if rotation is related to rib hump, what is causing the rotation and how does this relate to rib hump?
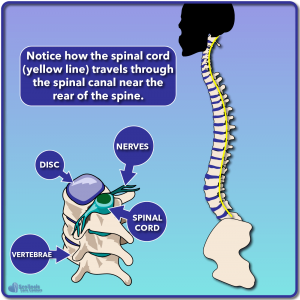
To understand rib hump, we first need to understand where the spinal cord is located relative to the spine. If you look at the image to the right (below on mobile) you can see that the spinal cord runs through the spinal canal which is located towards the rear of the spine (not down the middle of the spine). We also see how the spinal cord is flexible enough to travel along the normal curvature of the spine (ie. lordosis in the lumbar and cervical region).
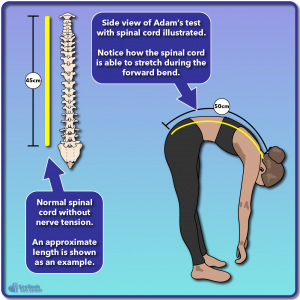
A normal spinal cord in the absence of nerve tension can flex and stretch as the body moves. As the body bends forward during an Adam’s forward bending test, the spinal cord will stretch to accommodate this movement. The spinal cord has been shown to stretch (elongate) by about 5-7 cm 1 when it is flexed; thus in this example we show a 45 cm long spinal cord stretching to be 50 cm during the Adam’s test.
Unfortunately, nerve tension can occur resulting in an effectively “shorter” cord. This idea is nothing new. In fact the idea that a short cord or nerve tension could cause scoliosis and a rib hump was first described in the 1960’s by Dr. Milan Roth 2, 3.
In the case of a short cord and nerve tension, we now have a shorter length cord and less “stretch” to work with as shown in the example to the right (below on mobile). The spinal cord will take the shortest path possible (the path of least resistance) in order to span the length of the spine as best as it can. The spinal cord is pulled even tighter when bending forward during the Adam’s test and as a result something has to give.
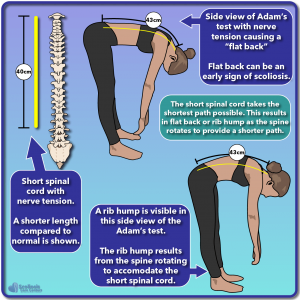
One possible result of our tight cord being pulled even tighter by bending over is something known as “flat back”. To escape the tension as much as possible, the spinal cord takes the straightest path possible. In our example we see the limited stretch lengthening our short cord from 40 to 43 cm, but because it is still short and tight, we lose the ability to bend over and flex normally.
Instead of causing flat back, another way the body can adapt to a tight/short cord is for the spine to rotate and collapse in order to provide the shortest path possible. Because the spinal cord runs down the spinal canal at the rear of the spine as we saw above, this rotation helps provide a shorter path for the cord to travel. Unfortunately, this nerve tension driven rotation and collapse result in a rib hump developing, and can also be the driving force behind a scoliosis.
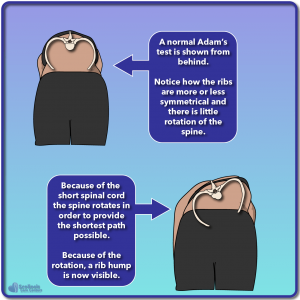
This concept can be better understood if we look from behind while performing the Adam’s test. Here we can see a normal Adam’s test result where no rib hump is present, the ribs are not distorted, and there is little rotation in the spine. However, once our spinal cord is short/tight due to nerve tension, we encounter rotation of the vertebrae to provide that short path. As a result of the rotation we see the rib cage begin to distort and we now see the rib hump used to identify a scoliosis.
It is important to notice that this rotation and rib hump can be present BEFORE a scoliosis has truly begun to develop. If tight nerves and a tight/short cord are present before periods of rapid growth (growth spurts) we may see a small rib hump adapting to the tight nerves. However because the spine and spinal cord have not begun to grow rapidly yet, we don’t see a large rotation and collapse into a scoliotic position. Thus, the Adam’s test seems to be a good test for underlying nerve tension which can ultimately result in a scoliosis developing over time. On the other hand, if we can treat nerve tension, stretch the spinal cord and nerves, and prevent the spine from rotating during growth with bracing, we can treat and even eliminate rib hump.
You can learn more about other methods to screen for nerve tension on our Early Detection page, and learn more about nerve tension causing scoliosis on our Treatment page.
References
- Breig, A. (1979): Adverse mechanical tension in the central nervous system, by Alf Brieg, Almquist & Wiksell, Stockholm, 1978, 264 pp, illustrated. In Annals of neurology 6 (5), p. 460.
- Roth, M. (1981): Idiopathic scoliosis from the point of view of the neuroradiologist. In Neuroradiology 21 (3), pp. 133–138.
- Roth, M. (1968): Idiopathic scoliosis caused by a short spinal cord. In Acta radiologica: diagnosis 7 (3), pp. 257–271.
Additional Scoliosis Treatment Results by Rib Hump Improvement and Stories