
Childhood Scoliosis: Causes and Progression
If you or your child has been diagnosed with scoliosis, the first and foremost thing to do is educate yourself on the topic to better guide your decision making for treatment.
“The better one’s understanding of a problem, the better their solution to the problem can be.”
What is Scoliosis?
Scoliosis can be defined as a combination of the following:
- A lateral bend in the spine. This is evident when viewing the spine from the front or back.
- A twist in the spine. The vertebrae are twisted out of their normal alignment.
- A loss of normal spinal curves when viewed from the side.

Does Adolescent Idiopathic Scoliosis have a Cause?
“Adolescent Idiopathic Scoliosis” Is an Incomplete Diagnosis
Many children with scoliosis receive the diagnosis of “adolescent idiopathic scoliosis.” But what does this term really mean?
Adolescent: A young person transitioning into adulthood
Idiopathic: Unknown cause or origin
Scoliosis: A three-dimensional deformity affecting the spine and trunk
Are There Types of Scoliosis? What’s Missing?
The label “adolescent idiopathic scoliosis” often marks the end of a diagnosis process. But this term simply means, “your adolescent has scoliosis, and we don’t know why.” It doesn’t explain the cause, which is critical for effective treatment.
When defining an illness, we don’t stop at not knowing the cause; we investigate further. Defining scoliosis should be no different: claiming we simply don’t know the cause and moving on is unacceptable. To define scoliosis means that we need to identify not only the signs and symptoms, but also the types and root causes for each type and each patient.
Some believe that “idiopathic” means there is no cause, but the spine twists and bends for a reason. The body always has a reason. Ignoring this cause overlooks the basic principle of cause and effect.
We believe that finding the reason for your child’s scoliosis is not only possible, but necessary. With modern science and a thoughtful approach, we can better understand and treat scoliosis. As Voltaire said, “No problem can withstand the assault of sustained thinking.”
What are the 3 Root Causes of Scoliosis?
1. Nerve Tension
Nerve tension scoliosis occurs when the spinal cord is tight, inelastic, or tethered, with nerve roots or meninges creating the force that causes the spine to coil into scoliosis. Nerve tension is likely to be one of the most common causes of scoliosis, especially when scoliosis progresses rapidly and is labeled “idiopathic.”
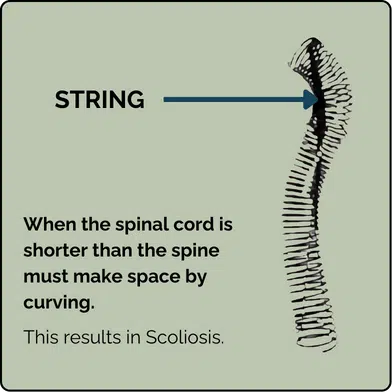
The Roth-Porter Hypothesis
The theory that a tight spinal cord could cause adolescent scoliosis was introduced by Dr. Roth in 1968 and expanded by Dr. Porter in 2001. They used the analogy of a spring with a string running through it: the spring represents the spinal bones, and the string represents the spinal cord. When the string is pulled tight, the spring coils, much like the spine does in scoliosis.
A common reason for nerve tension is Uncoupled Neuro-Osseous Development—when bones grow faster than nerves, leading to spinal cord or meningeal tension. This creates a tugging force on the vertebral column, causing it to compress and coil down into a scoliotic position. Scoliosis, in this case, is an adaptive response to relieve tension on the spinal cord.

Examples of Nerve Tension Pathologies Causing Scoliosis:
- Tumors or cysts: These can bind the meninges of the spinal cord, causing nerve tension. They may also create neuro-muscular dysfunction as described in root cause number 3.
- Intraspinal anomalies: The spinal cord or nerves develop embryologically in a way such that one side or one part of the cord is pulled tight at birth. This may not appear until growth spurts.
- Tethered Cord Syndrome: A congenital condition where the spinal cord is pulled lower toward the sacrum, placing tension on the spinal cord.
- Uncoupled Neuro-Osseous Development: The spinal cord is not growing as fast or as long as the bones of the spine. This is likely to become recognized as the most common cause of adolescent scoliosis.
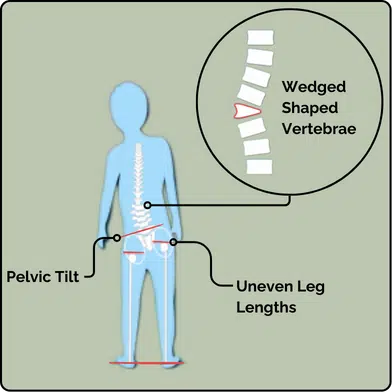
2. Structural Asymmetry
Structural scoliosis arises from issues with the bones or spine alignment. For example, a hemi-vertebra (half-formed vertebra at birth) can lead to scoliosis. Another common cause is leg length discrepancy, where one leg is slightly longer, causing the sacrum to tilt. Since the sacrum is the spine’s base, this tilt can result in a mild to moderate scoliosis. Structural causes may also stem from ligament damage due to trauma or disc degeneration. When stabilizing ligaments are compromised, the spine may tilt, leading to a scoliotic curve. These conditions are common and typically cause mild to moderate, non-progressive scoliosis.
3. Neuro-Muscular Pathology Causing Scoliosis
Neuro-muscular scoliosis occurs when there is a breakdown in the body’s control system (brain), the nerves connecting the brain to the muscles, or the muscles themselves. This results in scoliosis with a neuro-muscular cause. For example:
- Cerebral palsy: Impaired brain control affects muscle function.
- Poliomyelitis: Damaged peripheral nerves disrupt signals from the brain to the muscles.
- Muscular dystrophy: Weak muscles cannot support the spine.
These cases tend to be more severe, with a higher risk of scoliosis progression.
How does Scoliosis Progress?
Scoliosis rapidly worsens with growth. The most important thing to know about childhood scoliosis is that it worsens quickly during growth spurts. The faster a child grows, the faster scoliosis can worsen. This progression isn’t steady or linear—scoliosis can increase significantly in just a few months.
This rapid progression often leads parents to believe that scoliosis appeared suddenly. For example, a child may seem fine during a spring screening but develop a 40-degree curve by summer. In reality, the curve often begins long before it’s noticeable, but growth spurts cause rapid worsening, making the scoliosis more obvious.
Scoliosis Progression During Puberty
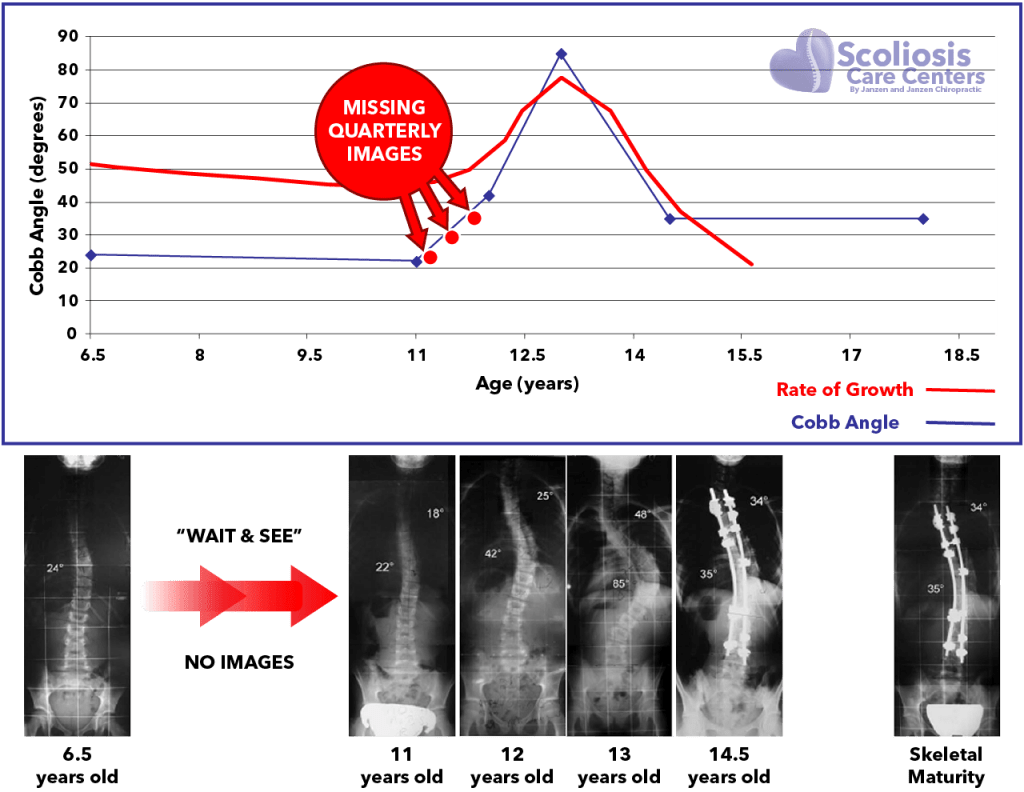
Scoliosis Progression and the Growth “Storm”
During rapid growth spurts, waiting 6 months to a year between X-rays may be too long. Significant worsening can happen in just a few months, so we recommend imaging the spine every 3 months or sooner if a child is growing quickly.
Why don’t most doctors image more frequently or when a patient grows?
- Radiation risk: X-rays expose children to harmful radiation, which has been linked to cancer in scoliosis patients. Protective measures like using lead shields for the breast, lungs, thyroid, and gonads are important.
- Surgical mindset: Many doctors believe that nothing can be done to stop scoliosis progression until it reaches the surgical threshold (40-50 degrees), at which point spinal fusion is often recommended.
What can you do to prevent rapid scoliosis progression?
- Quarterly Imaging with MRI: Use radiation-free, standing MRIs to track scoliosis progression. Standing MRIs are more accurate because they measure the curve under the force of gravity, providing a reliable and safe alternative to X-rays.
- Take Immediate Action: If your child is growing, using a highly corrective brace as soon as possible is crucial. Bracing full-time has been shown to significantly reduce the risk of scoliosis progression. Time spent without a brace during the growth period has been shown to result in 58% of high-risk cases worsening beyond 50 degrees and resulting in surgery.
- Monitor Growth Rate: Measuring growth monthly and watching for growth spurts will give a good indication of when a child is most at risk for getting worse. Notify your doctor if there has been a growth spurt!
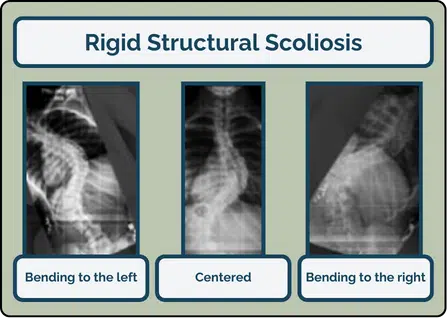
Understanding Scoliosis Progression: From Flexible to Rigid Curves
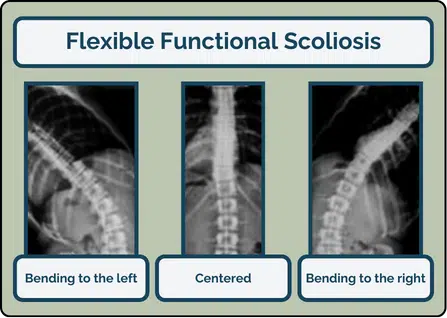
No matter the root cause, scoliosis typically begins as a small, flexible curve. At this stage, the spine can still move through its normal range of motion. In this flexible, or “functional,” scoliosis, lateral bending X-rays would show that the curve corrects easily when the spine is bent to the left or right.
As the curve grows, the soft tissues of the spine become distorted, leading to a loss of normal motion. Over time, this can result in severe stiffness and restricted movement.
Structural Scoliosis vs. Functional Scoliosis
Structural scoliosis refers to a curve that has become stiff and rigid, but this doesn’t mean it’s caused by structural asymmetry, like a wedge-shaped vertebra. It would be more accurate to describe it as “rigid” rather than “structural.”
Some doctors use the term “structural” to divide scoliosis into two categories:
- Functional scoliosis (flexible)
- Structural scoliosis (rigid)
However, most curves have both functional and structural aspects, making this distinction less clear. Using “structural” for rigid curves can also falsely suggest that the bones are misshaped, when in reality, most rigid curves involve minimal bone distortion. Additionally, the term often implies that surgery is the only option, which is not necessarily true.
How a Small Flexible Curve Becomes a Large Inflexible Curve
In child and adolescent scoliosis, a small flexible curve can quickly turn into a large, rigid one.
As the spine grows, tightness in the spinal cord causes the vertebrae to “coil down” like a spring. This leads to a scoliotic posture that the spine can’t straighten from, even when trying to bend. Over time, the ligaments, muscles, and discs stop moving through their normal range of motion, causing stiff “contractures” in the joints.
These contractured joints may feel like bone-on-bone, but it’s actually stiffened soft tissue. The good news is that soft tissue contractures can be loosened with proper mobilization. The bad news is that it is a difficult and arduous process to loosen up contractured soft tissue around the joints.
Events Occurring During Scoliosis Progression:
- Early Stage: Flexible, functional scoliosis
- Curve Progression: The curve size increases
- Loss of Range of Motion: Leads to joint contractures in the spine
- Stiff, Rigid Scoliosis: Becomes more “structural” and inflexible
- Bone Changes: Bones eventually change shape due to the stress, resulting in wedge-shaped vertebrae, asymmetric pedicles, and rib cage deformity
Bone Deformity in Scoliosis
In the early stages of scoliosis, most of the distortion occurs in the soft tissues. Over time, this can lead to changes in the shape of the rib cage. The vertebrae may become slightly wedge-shaped and asymmetric as scoliosis progresses.
Early Stage Bone Changes in Scoliosis
In the early stages of scoliosis, changes are most noticeable in the front part of the thoracic vertebrae. The front of the vertebra can grow taller than normal, a condition known as Relative Anterior Spinal Overgrowth. This overgrowth can lead to a loss of the normal thoracic curve, resulting in a “flat back.”
Late Stage Bone Changes in Scoliosis
As a scoliosis curve progresses, three key bone changes occur:
- The rib cage distorts to adapt to the growing curve.
- The pedicles of the spine may grow asymmetric in length and thickness.
- The vertebrae at the curve’s apex may develop a slight rhomboid-wedge shape, deviating from their normal rectangular shape.
Bone deformity is NOT most commonly what limits a spinal surgeon when straightening a spine. It is nerve tension from a tight spinal cord.
How Can You Detect Scoliosis Risk?
Now it is possible to catch the warning signs of scoliosis before a curve even begins. Learn about the Cox Test and how it may help you detect scoliosis early and potentially prevent surgery in a growing child.
References
- Dimeglio A, Canavese F. Progression or not progression? How to deal with adolescent idiopathic scoliosis during puberty. J Child Orthop 2013;7:43–9.
- Ylikoski M. Growth and progression of adolescent idiopathic scoliosis in girls. J Pediatr Orthop B 2005;14:320–4.
- Hoffman DA, Lonstein JE, Morin MM, Visscher W, Harris BS, Boice JD. Breast cancer in women with scoliosis exposed to multiple diagnostic x-rays. J Natl Cancer Inst 1989;81:1307–12.
- Simony A, Hansen EJ, Christensen SB, Carreon LY, Andersen MO. Incidence of cancer in adolescent idiopathic scoliosis patients treated 25 years previously. Eur Spine J 2016;25:3366–70.
- van Loon, Piet J M, Kuhbauch BAG, Thunnissen FB. Forced lordosis on the thoracolumbar junction can correct coronal plane deformity in adolescents with double major curve pattern idiopathic scoliosis. Spine (Phila Pa 1976) 2008;33:797–801.
- Auerbach JD, Lonner BS, Dean LE, Goldstein Y. The Feasibility of Radiation‐Free Diagnostic Monitoring in Adolescent Idiopathic Scoliosis using a Novel, Upright Positional MRI Protocol, E‐Poster #31. Spine Journal Meeting Abstracts 2009;10.
- Weinstein SL, Dolan LA, Wright JG, Dobbs MB. Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med 2013;369:1512–21.