Written and reviewed for scientific and factual accuracy by Dr. Austin Jelcick, PhD and Dr. Matthew Janzen, DC. Last reviewed/edited on October 28, 2020.
There are many animations of spinal fusion surgery available online as well as actual videos of surgery which describe what happens during spinal fusion surgery. While in actual videos of surgery it can be difficult to see what is happening, 3D animations of spinal fusion surgery can be quick to glance over major aspects of the surgical procedure without describing what happens. One area that is typically glanced over is the surgical release of soft tissues. This surgical release removes contractured ligaments and other soft tissue that limit how much the spine can be straightened. In addition to soft tissue, bone is also sometimes removed during this process to better allow the spine to be aligned to the surgically implanted metal rods.
This procedure is a part of the overall spinal fusion surgery, and can vary in its scope depending on how “stiff” the spine is. The stiffer the spine, the harder it is to straighten, and thus the more “release” is needed during surgery. This article will cover in detail what is performed during surgical release when spinal fusion surgery for scoliosis is performed. Specifically, this article and its accompanying infographic apply to what is done when spinal fusion is performed using posterior screws with a direct derotation of the vertebral bodies. Additionally, we also will talk about how “release” can be performed WITHOUT surgery, and also have a short video that demonstrates how this is achieved.
What happens before surgical release?
A surgeons’ goal during spinal fusion surgery for scoliosis is not only to straighten the spine as much as possible, but to prevent any further progression by surgically immobilizing the joints of the spine where the curve is present. This is done through the process of spinal fusion, which permanently eliminates movement in the joints through the use of bone grafts and surgical removal of various tissues.
For a posterior approach, the patient will be lying face down in the prone position and an incision is made in the back. The length of this incision depends on how much of the spine, or how many “levels” are to be fused. Once this is incision is made, pedicle screws are inserted into the spine. These screws ultimately attach to the inserted rods which force the spine into a straighter position.
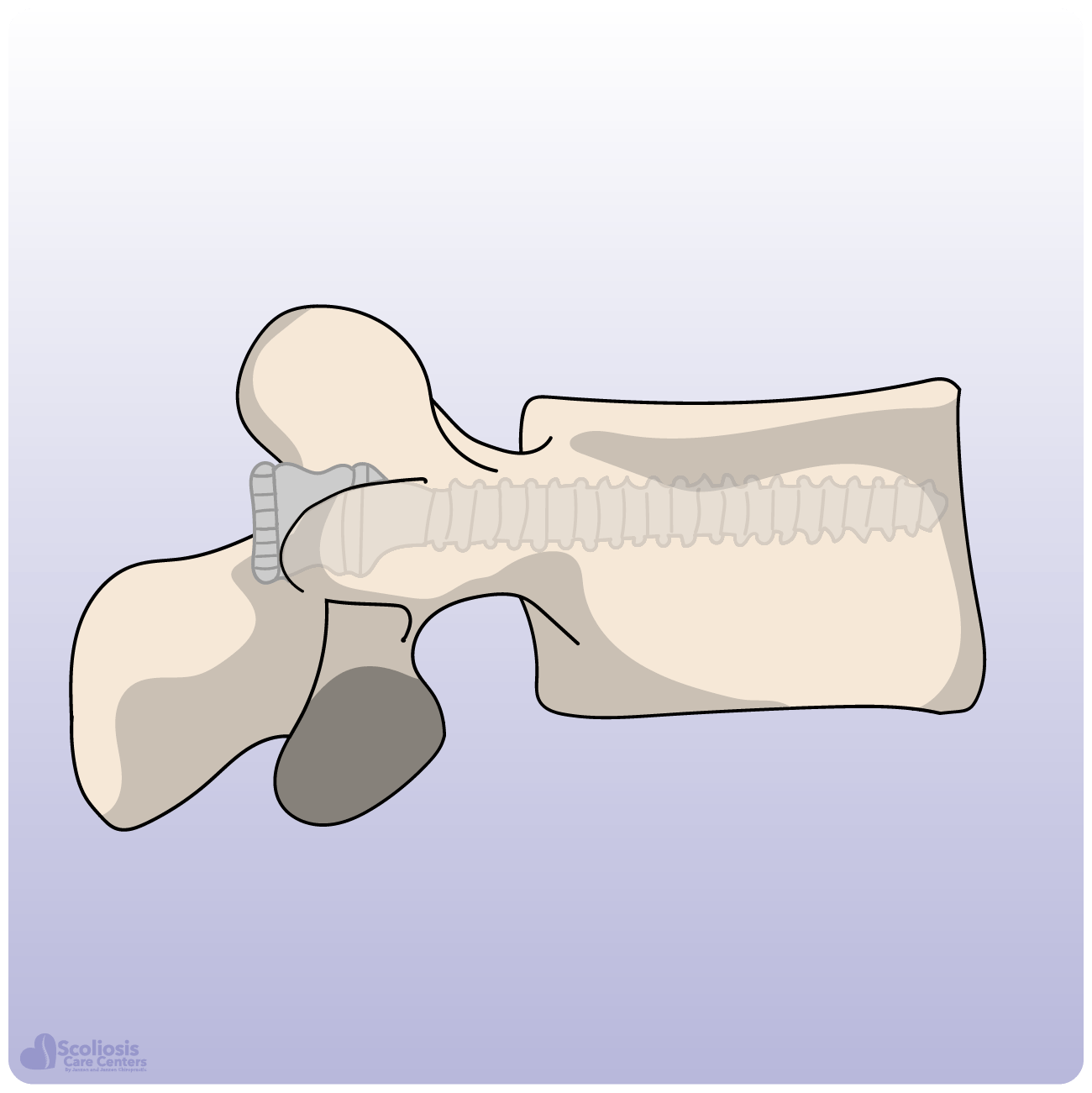
While the details of what happens during pedicle screw insertion are not covered in this article or infographic, you can see an example of how a pedicle screw is inserted into the vertebral body to the right (or below on mobile) as well as its relative size. One more thing to know about pedicle screws is that the number of screws used varies. Curves that are smaller and less “stiff” typically require fewer screws, while larger “stiff” curves require more.
How does a surgeon determine “stiffness”?
Before surgery ever occurs, a surgeon will try and determine how “stiff” the scoliosis curve is so that they have an idea about how much surgical release is needed. This is done using x-ray as the patient will have several x-rays taken where they bend to one side or the other. These are commonly known as lateral bending x-rays, and their purpose is to see if the curves reduce to any extent when bending from side to side, or if they remain virtually the same, indicating a “stiff” curve. You can see examples of these in the short video below.
The stiffer the curve, the more surgical release will need to be performed by the surgeon. If a curve is quite stiff, a fulcrum bending x-ray is performed where the patient is lying on their side with a pad/device placed underneath them which serves as a fulcrum that they bend over as shown in the image to the right (below on mobile). A traction x-ray while the patient is under general anesthesia can also be used to determine how stiff the spine/curve is.

What happens during surgical release?
Depending on how stiff the spine is found to be, the surgeon will perform release at anywhere from just the stiffest part of the spine (usually the apex of the scoliosis curve) all the way up to the entire length of the spine which is to have hardware implanted (the instrumented spine). Again, the surgeon performs release because the soft tissue and sometimes bone limits how much the spine can be straightened during surgery using the inserted rods and screws.
First, the surgeon will remove the inferior aspect of the spinous process. Next, they will also remove the interspinous ligament. If the surgeon requires even more release, bone is also removed by performing a Posterior Column Osteotomy, or PCO for short. This is also sometimes referred to as a Smith-Petersen osteotomy or a Ponte osteotomy.
Next, approximately three to five millimeters (3-5 mm) of the inferior aspect of the inferior facet joint is removed. This is done at each level of the spine which ultimately will be fused. The surgeon will also remove the ligamentum flavum, taking care not to penetrate too deep against the dura. The dura is the thick membrane that surrounds the spinal cord, making it very important to avoid so that neurological damage or paralysis do not occur accidentally.
Spinal surgery is a complex procedure and accidental tearing of the dura occurs in about 2.7% of spine surgeries4. If the dura is torn during surgery, it results in more complications (such as leaking of cerebral spinal fluid: CSF2), higher mortality rates, longer hospital stays, increased surgery cost, and a lower hospital discharge rate. A surgeon has to be particularly careful of this on the concave side of the scoliosis curve where nervous system tissues tend to be located.
After this has been performed, the surgeon will remove the top portion of the superior articular facet. This entire process is then repeated at each level of the spine as needed. With these steps now complete, the Posterior Column Osteotomy (PCO) is now complete, and the surgeon will proceed with performing fusion of the facet joints.
What happens during facet joint fusion?
When PCO has already been performed, the facet joints have already been removed during the steps described above. However, if PCO has not been performed because the surgeon did not deem it necessary, then the surgeon will proceed with performing fusion of each facet joint. First, the inferior articular facet is removed using a tool called an osteome, which looks somewhat like a chisel or flathead screwdriver as shown in the infographic. By doing this, the surgeon exposes the articular cartilage of the superior articular facet.
The surgeon will then remove this cartilage in preparation for the bone graft which will serve to immobilize the joint permanently. Pieces of bone graft are inserted into the facet joint, which will serve as a sort of scaffold for new bone growth. Bone grafts in spinal fusion surgery are typically obtained from the patients’ own bone elsewhere so that rejection is avoided and the graft will integrate successfully. Once healed, areas where bone graft were inserted will now be solid bone, effectively immobilizing the joint permanently and restricting/eliminating range of motion.
What happens after surgical release and fusion of the facet joints?
Briefly, once release and fusion of the facet joints has been performed, the surgeon will proceed with attempting to correct the scoliosis curve by inserting the rods. Rods are bent before insertion so that they provide the appropriate amount of “curve” to the spine (kyphosis and lordosis) depending on what region of the spine is having hardware inserted and being fused. The size of the curve, how stiff it is, and other variables are also taken into consideration to determine the amount the rods are bent.
Rods are inserted and as the spine is surgically derotated and straightened as much as possible, the rods are secured by the pedicle screws. Once the rods are in place and the spine has been surgically corrected, the final spinal fusion is performed. This fusion consists of removing the outer layer of the bone (decortication) followed by placement of bone grafts over the entire area of the decorticated spine. Lastly, if needed the surgeon can place additional transverse rod connectors to further stabilize the spine.
Is there an alternative to surgical release?
If the entire point of surgical release is to “free” the spine so that it is more mobile and able to be straightened, it makes sense that this might be able to be achieved without surgery. As we discussed earlier, a spine or curve being “stiff” is primarily caused by tight or stiff connective soft tissue. This stiff tissue is commonly known as contracture, and results from the spine being “stuck” in a curved position. You can learn more about contracture in other articles, but the key message is that contractures CAN be treated without surgery.
In joints other than those in the spine, contractures are routinely treated by physiotherapists using targeted prolonged stretching. This stretches the shortened tissue while also allowing the longer tissue on the other side to slowly return to its normal length as well. The video below goes into detail about contractures; how they occur in a spine with scoliosis; examples of bending x-rays which show how curves can be “stiff”; and most importantly, how contractures in the spine can be successfully treated without surgery.
By treating contractures, we effectively restore range of motion to the spine without destroying any of the joints or tissues which are removed during surgical release and fusion of the facet joints. This now allows the spine to be straightened more, improving how straight a brace can make the spine. We’ve talked before about how science shows the straighter the spine is in the brace the more successful treatment is, and how bracing has been proven to prevent surgery and reduce scoliosis curves. Thus, the successful non-surgical treatment of stiff contractured tissue is a key part to every non-surgical scoliosis success story.
Surgical Release Infographic

Embed this infographic
Want to share and embed this infographic on your blog or website? Just copy the code below:
<div style="clear: both;"><a href="https://scoliosiscarecenters.com/surgical-release-what-happens-during-scoliosis-spinal-fusion-surgery/"><img src="https://scoliosiscarecenters.com/wp-content/uploads/surgical-release-of-contractured-soft-tissue-and-facet-joint-fusion-spinal-fusion-surgery-8.png" alt="Surgical Release of Contractured Soft Tissue During Spinal Fusion Surgery for Scoliosis" /></a><br /><br /><a href="https://scoliosiscarecenters.com/surgical-release-what-happens-during-scoliosis-spinal-fusion-surgery/">Surgical Release: What Happens During Scoliosis Spinal Fusion Surgery</a> (Graphic) created by <a href="https://scoliosiscarecenters.com/">Scoliosis Care Centers</a> <em>Information and data obtained from AO Surgery Reference and PubMed; full references available in article.</em></div>
References
- AO Surgery Reference.
- Fang, Zhao; Tian, Rong; Jia, Yu-Tao; Xu, Tian-Tong; Liu, Yang (2017): Treatment of cerebrospinal fluid leak after spine surgery. In Chinese journal of traumatology = Zhonghua chuang shang za zhi 20 (2), pp. 81–83. DOI: 10.1016/j.cjtee.2016.12.002.
- Samartzis, Dino; Leung, Yee; Shigematsu, Hideki; Natarajan, Deepa; Stokes, Oliver; Mak, Kin-Cheung et al. (2015): Selection of Fusion Levels Using the Fulcrum Bending Radiograph for the Management of Adolescent Idiopathic Scoliosis Patients with Alternate Level Pedicle Screw Strategy. Clinical Decision-making and Outcomes. In PloS one 10 (8), e0120302. DOI: 10.1371/journal.pone.0120302.
- Yoshihara, Hiroyuki; Yoneoka, Daisuke (2014): Incidental dural tear in spine surgery. Analysis of a nationwide database. In European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 23 (2), pp. 389–394. DOI: 10.1007/s00586-013-3091-z.