Written and reviewed for scientific and factual accuracy by Dr. Austin Jelcick, PhD and Dr. Matthew Janzen, DC. Last reviewed/edited on March 10, 2020.
Genetic testing seems to be all the rage right now with Ancestry, 23andMe and many other providing insight into your family history and health using genetic testing. But what does it mean for a disease or problem to be genetic? Is scoliosis hereditary or is it genetic or is it both? When searching for answers for these seemingly simple questions there are mountains of jargon to contend with and an almost equal amount of misinformation being spread by everyone under the sun who is trying to sell “genetic treatments.”
We’ve written this article as both an introduction and primer for genetics, as well as what we hope is a clear answer as to what science says on the matter. The short answer is this: scoliosis does have a genetic component, and scoliosis can be hereditary and run in families. However, as is often the case with health, the answer is not that simple. Scoliosis can be hereditary but it can also appear in families with no history of scoliosis. But that does not mean genetics don’t play a role in a curve developing or getting worse.
Genes, SNPs, DNA, RNA: What does it all mean?
The world of genetics is full of jargon and abbreviations that can quickly seem like an entirely different language. However understanding the fundamentals of genetics and how letters of DNA code can result in your hair being brown isn’t too hard at all. A good way to think about genetics is like a book, and in this case that book is you.
The Genome
You are the book, meaning that filled within the pages of the book are the billions of letters of DNA in your genome. The “book” is your complete genome: it has all of the information for every type of cell in your body to grow, develop, and function as they should. DNA can be thought of as the letters that make up your entire book. There are a set number of letters (26 letters in the English alphabet, and 4 letters, aka bases in DNA), and with that small number of letters, you can write an almost infinite number of books each as different or similar as you would like. So the order of the letters, or the DNA code determine the final book, but there is more to it than just this.
All of the DNA “code” that makes up your genetic “book” is your genome
Genes
We can think of genes as “words” in our book. Each has its own purpose or function, but there are many words that are similar to one another. Just as there are different versions of “there”, “their”, and “they’re” each with its own meaning, so too can there be similar genes with different functions. Take Collagen for example: there are a number of different versions of collagen, all similar, yet some with different functions or roles. In this example we have different variants and types of collagen, and each play their own role or biological function in the body, even when they are highly similar.
When we get a bunch of genes that work together for one larger purpose, now we have a “pathway.” In our book you can think of this like types of words. Running, jogging, swimming, flying…all of these you might call words involved with movement: the movement “pathway.” Similarly there can be multiple (sometimes hundreds) of genes working together in one big pathway such as the production of Estrogen.
Different genes can work together in groups known as pathways
The big important thing to remember about gene pathways is that they work a lot like a group project. If one person in the group isn’t doing their job (one gene isn’t functioning correctly) it can sometimes not matter much. Other people in the group will pick up the slack, and the project still gets done; maybe not as good as it could have been but it’s still good. On the other hand, sometimes an important member of the group can fail at their job and the entire project can be ruined. The point is, problems can happen in different genes or parts of a pathway with different results and sometimes what you think is the problem is just the EFFECT of a problem elsewhere. In our group project for example, the group member in charge of printing could not do their job, but only because the person in charge of writing the report didn’t do theirs. Even though it would appear the printer didn’t do their job, it was due to a different problem “upstream” of them.
Introns
Now you may have heard of “non-coding” DNA or an Intron as its commonly known. These used to be thought of as “junk DNA” and in the case of our book, you can think of introns as all the blank space that separates our words: the spaces, the paragraph breaks, even the blank pages. While the space is blank, there is still meaning to the space; the same is true of introns. If you delete a space in your book where there should be one, or remove a blank page, the book will read differently.
Introns aren’t genes but still contain important genetic information
If we remove a space somewhere in our book, a sentence might be hard to understand or two words may now be combined to make nonsense. The same goes for introns. Often there are important things in this DNA code, things that help understand the “book” correctly such as biological signals of where to start or stop reading and more. Needless to say you can have a mistake in your “blank” space and still mess up your book even though you didn’t make a mistake in the letters or words.
SNPs
Services like Ancestry and 23and me use little parts of the genome, of your book, to identify you and see who you are related to and how far back your family tree stretches. These are the same little parts that they use in law enforcement and on an episode of CSI to identify the bad guy from their DNA (as well as other genetic elements like short tandem repeats). These little parts are commonly known as SNPs, and in our book you can think of them as little typos in the text.
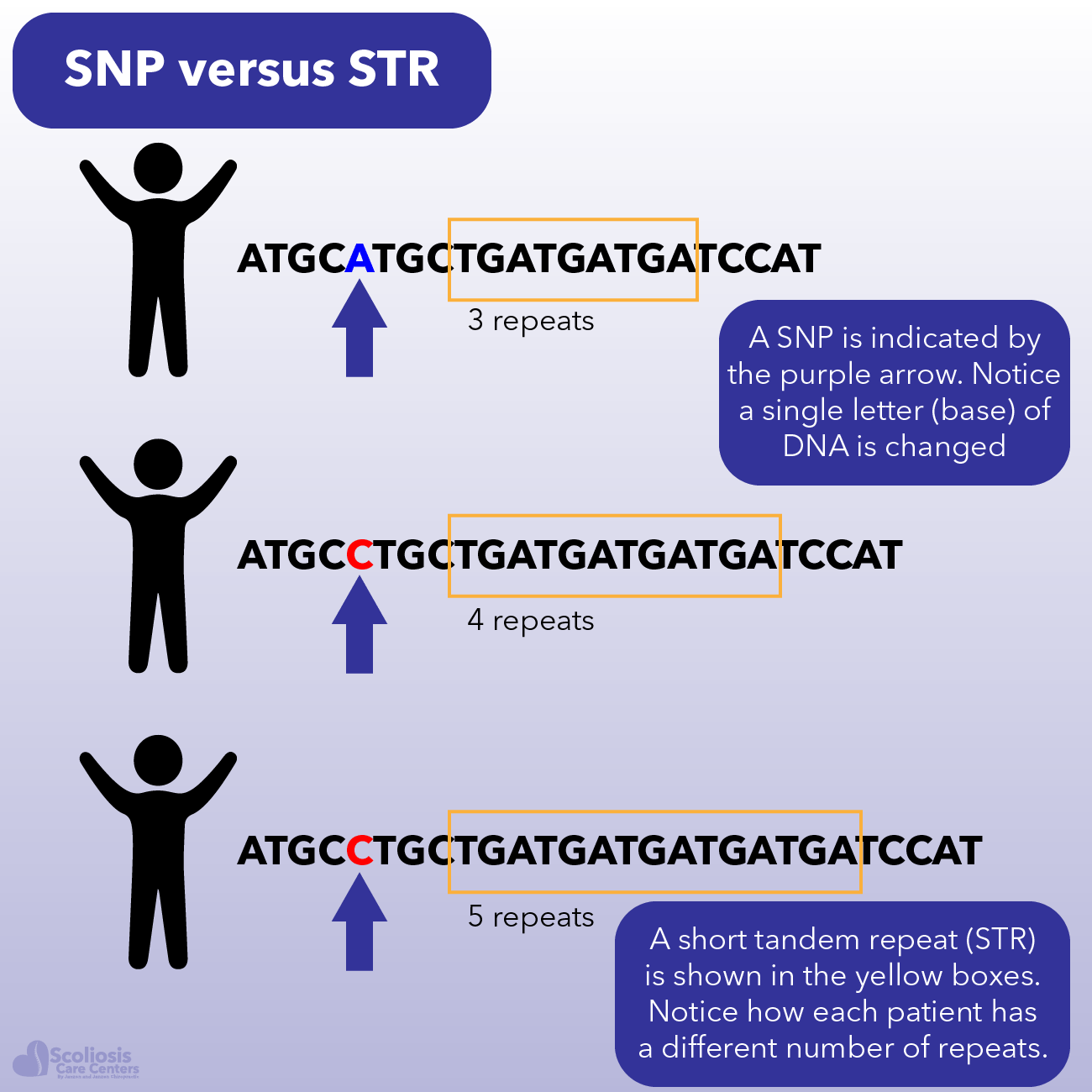
Take this word for example: sustainibility. You probably read it correctly, and may not have even noticed the misspelling where there is an “I” where an “A” should be. Here we have a SNP: an I where there should have been an A, but the word still makes sense, and most people reading it may not even notice and still read the book just fine. In this case we would call this a “silent” SNP because it didn’t change our word or its meaning much and things continue as normal.
A SNP is a tiny variation in your DNA that can also be associated with disease risk
We all have thousands of silent SNPs in our genome. Where these SNPs are and how they are different helps make up a profile that can be used to identify us. But sometimes typos are worse, and SNPs can be to. For example, look at this word: suttain. Without knowing it is a misspelling of “sustain” you might have trouble understanding the word; the meaning of the sentence; or the paragraph it is in. When these types of typos or SNPs happen, problems can occur because now our genetic code (our book) is not being read correctly. Depending on what has happened (ie. a missing letter, and extra letter, etc.) the effect can be different. This is one reason why you can find two people with the same disease, yet one is more severe than the other because they have different “typos” in their genome. Even when the same “word” or gene has the mistake, where and what kind of mistake is there can make a big difference.
One more quick word on SNPs: association. We talked about how SNPs can be made into a “profile” to identify you in CSI and discover your great great grandmother. However, SNPs can also be used to discover patterns in diseases like scoliosis. While these SNPs may not be the REASON that the disease is there, they can be ASSOCIATED with the disease and with the RISK of the disease or the disease getting worse.
A large number of scientific studies look at risk factors associated with disease, and you have probably heard a news story where “scientists find genetic risk factor for disease X.” It is quite common for people with certain SNPs to have a higher or lower risk for something, even though that “thing” is not caused directly by their SNPs. What the SNPs give us is something to look for to gain a better idea of what RISKS are present.
Transcription and Translation
Our book is our genome, and it’s made up of genes, SNPs, introns, and more. But how the book is read is just as important as what is written in the book. For example, if we open to page 17 and start reading, the story might not make sense compared to if we started on page 1 as we should have. The act of “reading the book” or reading the DNA code is known as transcription and there are little parts of the genome that tell the cells and body where to start and stop reading; just as in a book there are chapters and paragraphs so you know where to start and stop. If we mess up one of these little cues as to when to start or stop reading, our story can stop making sense and we can have a problem (ie. disease or birth defects).
Even if a gene is normal problems can happen when the gene is “read” or transcribed by the body
The other step of transcription is converting DNA to RNA: in this case mRNA which is known as messenger RNA and for good reason. Transcription isn’t just reading the book, its also copying the book into a short message that we can use. In this case imagine our book is actually a cookbook. You have the recipes for every kind of food in your book, but you only need the recipe for chocolate chip cookies right now. Similarly, your whole genome isn’t needed all the time and your cells may just need to make more collagen. So we read the book (our genome) and transcribe the message only for chocolate chip cookies (the gene we want to transcribe), and only when we need it. So now we have our recipe out of our book but we still need to make our cookies.
This is where translation comes in. If transcription is reading the part of the book we need to get the recipe we need, translation is making the recipe. In biology, this is the part where the messenger RNA (mRNA) is read and the protein is made. A protein is made up of different amino acids, and the message of our mRNA determines what peptide or protein will be made. During translation different amino acids are joined to make a long string (a peptide) and if that string is long enough, we stop calling it a peptide and now call it a protein. While changes can be made to the protein later (something known as post translational modification), the important thing to understand here is that just as a mistake can happen in our book, as well as when we read our book (transcribe) mistakes can also happen when we make our recipe (translate).
Putting Our Cookbook To Use
We’ve gone over the basis of genetics and how your genome is used to make all the proteins your body needs just as our book is read and then transcribed into the message we needed to make our recipe. One more thing to keep in mind is that just as not every recipe is used everyday, the different cells of your body make different proteins and do so at different times of development and even during the day.
How much or how little a gene is expressed can vary depending on the cell, development, time and more
Genes involved in your circadian rhythm (the day/night cycle that regulates your sleep) change in expression throughout the day, while others change as we grow, and even others still can change in expression based on our environment. As an article in The Atlantic described multiple studies, identical twins may have the same genetic code (the same book) but how their genes are expressed (how the book is read) can vary and be influenced by the environment.
This again is important because it lets us know that we can have two identical people, with the same risk factors, but they can have different outcomes based on their environment. For example, we could have two twins who are extremely skinny and have genetics that give them a faster metabolism than normal, but if one of them eats fast food for every meal, they likely will not look the same or have the same health as their non-fast food eating twin.
Genetic Misinformation
If you look for information about scoliosis and if it is genetic or hereditary or both, you likely will come across a few very misleading articles. Terminology is used inappropriately and in a way that is not only confusing, but that can be misleading. For example, one article claims that something can be genetic without being hereditary, and that something can be hereditary without being genetic. If we were discussing politics or family recipes this might be true: things that are passed down from generation to generation like a family recipe could be called “hereditary” even though it isn’t genetic.
If something biological is hereditary it is also genetic
Genetic Inheritance
In biology and genetics, if something is passed down from parent to child, it is hereditary and this BECAUSE it is genetic. A child receives one copy of their chromosomes from their father and one copy from their mother. While their expression can vary and there are a wide number of genetic diseases and issues that can occur where genetic information is lost, changed, or gained, the genetic “book” that makes up a child’s genome is something they inherit from their parents.
Just because a parent has a disease doesn’t mean that their child will always have it though, as a parent’s genetic information is “mixed up” each time their body makes an egg or a sperm so that the child isn’t completely 50% identical to their parent. Similarly, the PATTERNS of genetic inheritance can vary and have wonderfully complex names such as autosomal dominant, or dominant negative. However if a parent has a risk factor or a disease, there is a chance that the child could have it despite the “genetic shuffle” that happened before they were conceived.
Germline What?
The claim that something can be genetic without being hereditary is at its core a misunderstanding of the correct terms. Let’s say for example that we have a mutation in our DNA that causes our hair to be blue. If this mutation had happened in the sperm or egg that combined to make the child, this would be known as a GERMLINE mutation. So if there is a genetic “typo” in the DNA of the sperm or egg, after they combine and develop and the child is born, every copy of the child’s DNA will have that genetic typo as well because it was present in one of the original cells they developed from: the sperm or the egg. There are some exceptions to this (for example when a disease is called “mosaic”) but that is outside the scope of this article.
Genetic changes can be both hereditary (germline) and non-hereditary (somatic)
On the other hand, genetic typos and mutation can happen after a child is born. Take smoking for example. If you smoke cigarettes, there are carcinogens in the cigarette that can damage DNA and cause cancer. While you are still causing a genetic typo due to the chemicals in the cigarette affecting DNA, this isn’t because of the sperm or egg, and this isn’t happening in EVERY cell of the body. Thus this type of mutation is known as SOMATIC mutation.
Understanding these terms and their differences is important because over simplifying and saying something can be genetic but not hereditary adds more confusion than clarity. As with anything health related, if you understand the issue better you can make more well informed decisions instead of allowing someone to potentially mislead you.
Functional Groups
We already discussed genes, introns, SNPs, and how genes can be grouped into pathways even when they already have variants of their own (ie. collagen). With this understanding of genetics it is easy to see why some information can be misleading as various groups and clinics talk about “functional groups” of genes. Often times these “groups” are nothing more than different versions of the same gene.
While this may seem like a technicality, it becomes important because multiple genes can have similar functions and be involved in the same pathway despite having different names. Thus, what may seem like several different “functional groups” as described by one clinic may in fact be a number of interconnected genes that are all involved in the same pathway and work together and therefore need to be thought of as a connected group. A good way of thinking about this is someone could say they can’t eat cheese, milk, or ice cream because those three food groups cause them problems. Instead of trying to figure out why each of those are causing a problem you should realize they are all members of the dairy family (the same “pathway” in our example) and need to be addressed as a group to get to the root of the problem.
Our Collective Knowledge of Genetics
One article that talks about if scoliosis is hereditary or genetic tries to make the claim that because a certain number of cases of scoliosis go to surgery, and because a much smaller number of cases are due to genetic risk factors, the rest of those cases must be due to the environment. This logical jump to conclusions not only is a gigantic fallacy, but a statement that cheapens the advancements made in genetics in the last 20 years.
The genes and risk factors associated with scoliosis are still being discovered
The human genome was only sequenced for the first time within the last 20 years, and while our understanding has exploded since then we still don’t understand a lot about it. Take introns for example. As we discussed, these used to be thought of as “junk DNA” that had little to no purpose. Yet now we understand that there are important things hiding in introns that regulate our genome. In fact this now has its own entire fields of study such as epigenetics and transcriptomics.
Thus, to say that only 1% of idiopathic scoliosis cases are due to known genetic causes while the remainder is due to environment is simply wrong. In all likelihood we will continue to discover new genetic risk factors that together cause or contribute to a scoliosis curve. While environment DOES play a role (environment affects how your genes are expressed), there are likely many more genetic and environmental factors and relationships to discover. Latalski et. Al put it very nicely when they said that “scoliosis is a multifactorial condition with genetic predisposing factors is apparently the closest to the truth.” 1
Is Scoliosis Hereditary?
Now that we have talked about what it means for something to be hereditary; how genetics are passed down; and how genetic problems can occur that aren’t passed down, let’s talk about heredity. Research has found numerous genetic factors associated with scoliosis, risk, progression and more. However, taken together it is clear that there is not one single gene or factor at work causing scoliosis. This is why the development of scoliosis has been termed “multifactorial”, meaning multiple factors play a role in its development.
Are You Born With Scoliosis?
While scoliosis only occurs in a small portion of the population the majority of cases of scoliosis are deemed idiopathic because they cannot be traced to a single cause. In fact, 70-90% of cases are deemed idiopathic.2 While scoliosis can be present at birth in cases of congenital, neuromuscular, and syndromic scoliosis, this is often not the case for idiopathic scoliosis. While it is widely accepted by the scientific community that genetics certainly play a role in the development of scoliosis 3, only about 11% of first degree relatives (ie. siblings, parents) are affected by scoliosis if another first degree relative has a curve 4.
This number decreases for second degree (2.4%) and third (1.4%) degree family members. So while it is possible to be born with scoliosis, for most cases of idiopathic scoliosis this isn’t the case but instead the curvature of the spine develops over time due to genetic and environmental factors with the cause being deemed “unknown”; thus the diagnosis of “idiopathic” which is defined as a disease that “arises spontaneously or for which the cause is unknown.”
How Is Scoliosis Genetic? Is There a “Scoliosis Gene”?
While science has not found a single “scoliosis gene” that can be passed down, research has found many different genetic factors and variants that seem to contribute to a scoliosis curve developing. As you would imagine, the genetic factors have been found to vary from population to population and there is still debate regarding whether these genetic factors are present in all populations.
Multifactorial: something that has multiple contributing factors
For example, we know that scoliosis happens far more often in girls than boys and as such, it was discovered that there is a part of the X chromosome (the female sex chromosome: women are XX and men are XY) which may be linked to familial (inherited from parents) idiopathic scoliosis 5. However there have been many other studies that discovered DIFFERENT genetic factors associated with idiopathic scoliosis, supporting the idea we’ve talked about that scoliosis has many contributing factors (is multifactorial).
If you recall from our genetics discussion that when we “read our book” and transcribe DNA to mRNA, there can be problems that can arise during transcription; one study found that there seems to be abnormal expression of mRNA (and other types of RNA) in patients with adolescent idiopathic scoliosis 6. Another study found that there may be a problem with transcription (reading our genetic “book”) of several genes (ie. TGFB2, TGFB3). Additionally, other genes which act in response to these can have their expression altered. It was found that the levels of transcription and the levels of expression of those responsive genes varied depending on the side of the curve (left or right) as well as how old the child was when the curve appeared 7,8.
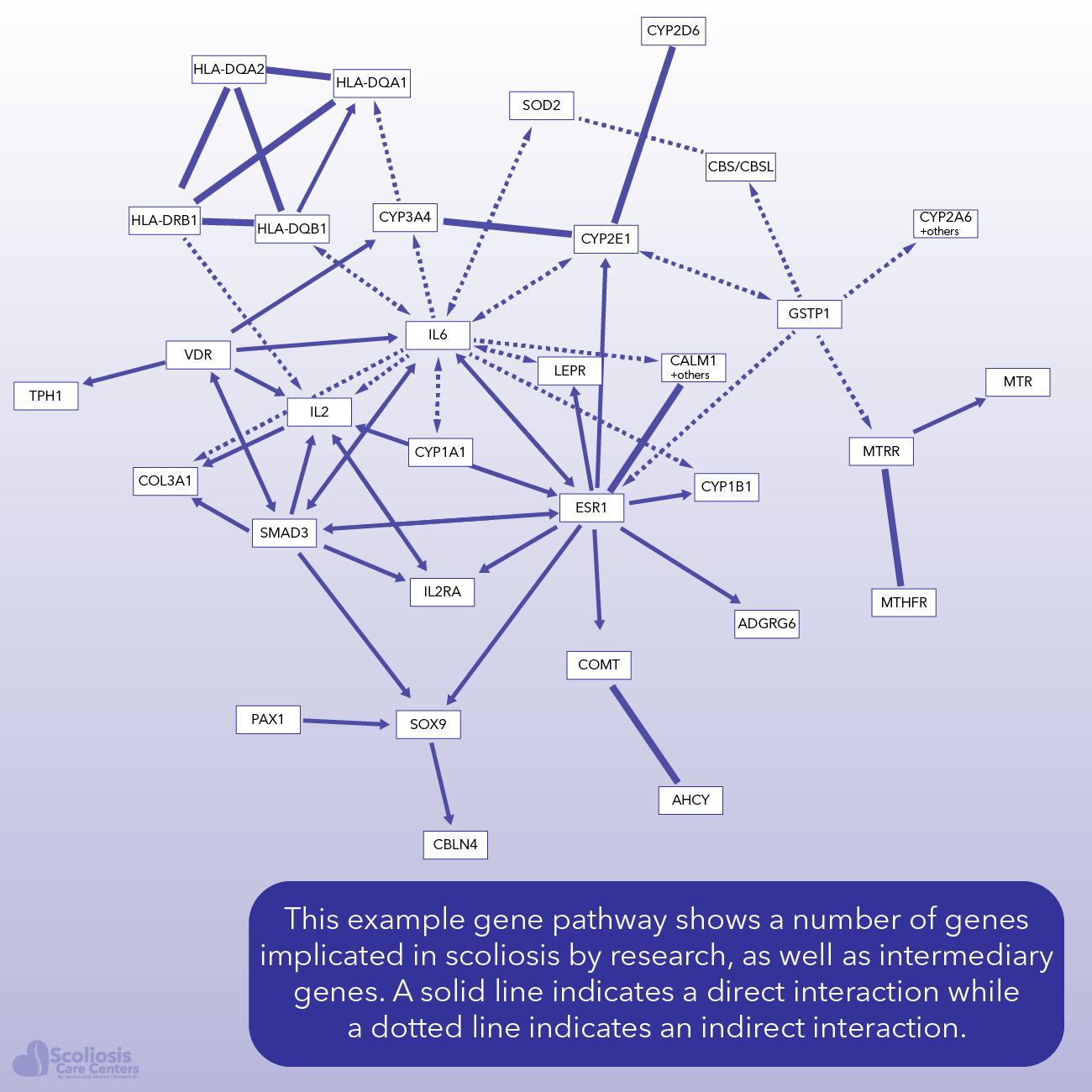
To add to the complexity of idiopathic scoliosis and its genetic risk factors, other studies found various genes and SNPs associated with idiopathic scoliosis including GPR1269; CHL1, ROBO3, and DSCAM10; SOC3, PTP-1B, and SH2B111; VDR17; PRMT5, COLX, MMP13, RUNX212 and more. Rather than chasing individual genes or SNPs some scientists have taken a more “top down” approach and have looked at entire genetic PATHWAYS and have found that certain pathways appear to be altered in idiopathic scoliosis.
Numerous genes and risk factors have been associated with scoliosis
In biology when cells “talk” to one another using molecules it is known as “signaling” and one study found that the signaling pathway related to Leptin (a hormone that helps regulate our hunger) is important in the development of scoliosis 13. Other pathways including axon guidance 10, growth hormones 14,15, and estrogen 16,17 have also been implicated in the development of scoliosis. In fact, if we look at a number of genes found in the research that are involved in scoliosis we find that quite a few are connected in a pathway to ESR1: an estrogen receptor.
Can The Environment Affect Scoliosis?
We know that the expression of genes can vary depending on the environment. Even identical twins can differ in how their genes are expressed despite having identical genomes 18. As we talked about before, changes to the genome can happen AFTER you are born and these changes are not always passed down as they can be SOMATIC changes. Just as identical twins can now be distinguished genetically through these somatic mutations 19, somatic mutations can alter gene expression and thus change ones risk for getting a given disease resulting in even identical twins having different risks for disease. While environmental factors like carrying a heavy backpack have not been found to cause scoliosis 20, the environment can still affect how genes are expressed.
Nature versus nurture: the environment can affect how our genes are expressed
Considering how complex the growth of the spine and spinal cord are, and also that during the adolescent growth spurt a child is most susceptible to their curve progressing 21, it certainly is reasonable that the environment can affect the development of scoliosis as it does seem to contribute to the progression of a curve 1.
Tying It All Together
Dr. Roth and Dr. Porter have previously described idiopathic scoliosis as being the result of underlying nerve tension as a result of something called asynchronous neuro-osseous growth. A situation where the spine grows faster than the spinal cord can keep up with, and as a result nerve tension results with scoliosis developing as an adaptation to the short cord. While we have talked about this in previous articles and how it also relates to a curve worsening with growth, as you would imagine everything we have talked about here relating to genetics and heredity play a role as well.
If you recall, we talked about a study which found changes in gene pathways related to axon guidance. Axons have to do with neurons and the nervous system, and so if we have a problem with correct axon guidance, we can encounter issues with the proper development of the nervous system. While this pathway has not yet been shown to be directly related to Dr. Roth and Dr. Porter’s findings, the research certainly goes hand in hand.
Multiple gene pathways are involved in normal development of the spine and nervous system
There are a large number of genetic pathways that are related to proper development of the spine and bone as well as the spinal cord and the nervous system. These pathways involve numerous genes, introns, SNPs, and more. Each of these genetic components that are involved in normal development can have mutations or variants which increase risk, and as you would expect there can be multiple issues that occur that each contribute to a bigger problem.
So while there isn’t one “scoliosis gene” we are looking for, we know that we need to be looking at the bigger picture. There are likely numerous problems that contribute to the spine growing faster than the spinal cord, and it is quite likely that there are issues in different parts of each pathway that result in scoliosis. After all, research has found different genetic changes in different patient groups 22, showcasing the variety of genetic problems that can all result in a scoliosis developing.
Scoliosis is multifactorial and involves multiple genes 23. However, these numerous genetic factors don’t exist by themselves but instead work together in different pathways to regulate and help the body develop. Problems can arise at different places in each pathway, and as a result the final outcome can vary. Just as one sibling may have a curve and the other does not, in other situations one curve may get significantly bigger while another doesn’t.
Scoliosis can be hereditary, and it certainly has associated genetic factors. New research continues to discover new genes, SNPs and other genetic elements associated with the development of scoliosis. As we learn more about scoliosis through rigorous scientific study, we can better understand all the pieces of the puzzle and how they fit together, allowing for the development of new treatments to address each problem wherever it may occur.
References
- Latalski, M. et al. Current insights into the aetiology of adolescent idiopathic scoliosis. Archives of Orthopaedic and Trauma Surgery 137, 1327–1333; 10.1007/s00402-017-2756-1 (2017).
- Letellier, K. et al. Récents progrès dans l’étiopathogénie de la scoliose idiopathique de l’adolescent et nouveaux concepts moléculaires. Medecine sciences : M/S 23, 910–916; 10.1051/medsci/20072311910 (2007).
- van Rhijn, L. W., Jansen, E. J., Plasmans, C. M. & Veraart, B. E. Curve characteristics in monozygotic twins with adolescent idiopathic scoliosis. 3 new twin pairs and a review of the literature. Acta orthopaedica Scandinavica 72, 621–625; 10.1080/000164701317269058 (2001).
- ROAF, R. THE TREATMENT OF PROGRESSIVE SCOLIOSIS BY UNILATERAL GROWTH-ARREST. The Journal of bone and joint surgery. British volume 45, 637–651 (1963).
- Justice, C. M., Miller, N. H., Marosy, B., Zhang, J. & Wilson, A. F. Familial idiopathic scoliosis. Evidence of an X-linked susceptibility locus. Spine 28, 589–594; 10.1097/01.BRS.0000049940.39801.E6 (2003).
- Liu, X.-Y., Wang, L., Yu, B., Zhuang, Q.-y. & Wang, Y.-P. Expression Signatures of Long Noncoding RNAs in Adolescent Idiopathic Scoliosis. BioMed research international 2015, 276049; 10.1155/2015/276049 (2015).
- Nowak, R., Szota, J. & Mazurek, U. Vitamin D receptor gene (VDR) transcripts in bone, cartilage, muscles and blood and microarray analysis of vitamin D responsive genes expression in paravertebral muscles of juvenile and adolescent idiopathic scoliosis patients. BMC musculoskeletal disorders 13, 259; 10.1186/1471-2474-13-259 (2012).
- Nowak, R., Kwiecien, M., Tkacz, M. & Mazurek, U. Transforming growth factor-beta (TGF- β) signaling in paravertebral muscles in juvenile and adolescent idiopathic scoliosis. BioMed research international 2014, 594287; 10.1155/2014/594287 (2014).
- Kou, I. et al. Genetic variants in GPR126 are associated with adolescent idiopathic scoliosis. Nature genetics 45, 676–679; 10.1038/ng.2639 (2013).
- Sharma, S. et al. Genome-wide association studies of adolescent idiopathic scoliosis suggest candidate susceptibility genes. Human molecular genetics 20, 1456–1466; 10.1093/hmg/ddq571 (2011).
- Burwell, R. G. et al. Pathogenesis of adolescent idiopathic scoliosis in girls – a double neuro-osseous theory involving disharmony between two nervous systems, somatic and autonomic expressed in the spine and trunk: possible dependency on sympathetic nervous system and hormones with implications for medical therapy. Scoliosis 4, 24; 10.1186/1748-7161-4-24 (2009).
- Liu, Z., Ramachandran, J., Vokes, S. A. & Gray, R. S. Regulation of terminal hypertrophic chondrocyte differentiation in Prmt5 mutant mice modeling infantile idiopathic scoliosis. Disease models & mechanisms 12; 10.1242/dmm.041251 (2019).
- Liang, G. et al. Normal leptin expression, lower adipogenic ability, decreased leptin receptor and hyposensitivity to Leptin in Adolescent Idiopathic Scoliosis. PloS one 7, e36648; 10.1371/journal.pone.0036648 (2012).
- Allen, D. B. Safety of human growth hormone therapy. Current topics. The Journal of pediatrics 128, S8-13; 10.1016/s0022-3476(96)70003-3 (1996).
- Ahl, T., Albertsson-Wikland, K. & Kalén, R. Twenty-four-hour growth hormone profiles in pubertal girls with idiopathic scoliosis. Spine 13, 139–142; 10.1097/00007632-198802000-00001 (1988).
- Lahmar, S., Kessabi, K., Banni, M. & Messaoudi, I. First evidence on protective effect of exogenous melatonin supplementation against disruption of the estrogenic pathway in bone metabolism of killifish (Aphanius fasciatus). Fish physiology and biochemistry; 10.1007/s10695-019-00748-w (2019).
- Leboeuf, D., Letellier, K., Alos, N., Edery, P. & Moldovan, F. Do estrogens impact adolescent idiopathic scoliosis? Trends in endocrinology and metabolism: TEM 20, 147–152; 10.1016/j.tem.2008.12.004 (2009).
- Choi, J. K. & Kim, S. C. Environmental effects on gene expression phenotype have regional biases in the human genome. Genetics 175, 1607–1613; 10.1534/genetics.106.069047 (2007).
- Budowle, B. Molecular genetic investigative leads to differentiate monozygotic twins. Investigative genetics 5, 11; 10.1186/2041-2223-5-11 (2014).
- Ghanem, I. & Rizkallah, M. Adolescent idiopathic scoliosis for the primary care physician. Frequently asked questions. Current opinion in pediatrics 31, 48–53; 10.1097/MOP.0000000000000705 (2019).
- Weinstein, S. L. & Ponseti, I. V. Curve progression in idiopathic scoliosis. The Journal of bone and joint surgery. American volume 65, 447–455 (1983).
- Alden, K. J. et al. Idiopathic scoliosis. Identification of candidate regions on chromosome 19p13. Spine 31, 1815–1819; 10.1097/01.brs.0000227264.23603.dc (2006).
- Czeizel, A., Bellyei, A., Barta, O., Magda, T. & Molnár, L. Genetics of adolescent idiopathic scoliosis. Journal of medical genetics 15, 424–427; 10.1136/jmg.15.6.424 (1978).