Written and reviewed for scientific and factual accuracy by Dr. Austin Jelcick, PhD and Dr. Matthew Janzen, DC. Last reviewed/edited on October 28, 2020.
What exactly is adolescent idiopathic scoliosis? Adolescent Idiopathic Scoliosis (AIS) is an abnormal curvature of the spine exceeding 10 degrees, diagnosed in adolescence and in which the cause is unknown. The deformity occurs with rotational misalignment, often marked by a hump in the ribs or low back, as well as loss of the normal sagittal curves of the spine:
Adolescent
The diagnosis is made in adolescence.
Idiopathic
The reason for the scoliosis has not yet been determined. The term “Idiopathic” comes from Greek and literally translated would mean “one’s own private suffering”. A case will be labeled “idiopathic” if there are no obvious neuromuscular diseases, genetic syndromes or congenital malformations.
Scoliosis
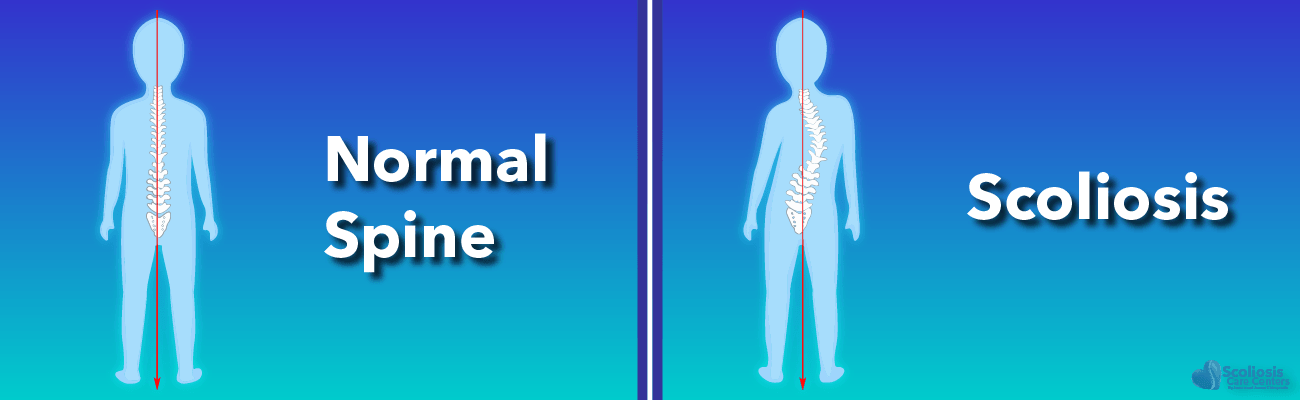
Three-dimensional deformity of the spine marked by both curvature beyond 10 degrees as well as a twist.
Misuse of the “Adolescent Idiopathic Scoliosis” Diagnosis
In practice, AIS is used as a final diagnosis for adolescent scoliosis with a specific, recognizable pattern of symptoms. Rather than as an admission we don’t have a diagnosis yet, AIS is being treated as the diagnosis. When one receives the diagnosis of AIS, it should mean that the doctors have more work to do in an effort to understand the cause of the curve. That being said, the types of cases that end up in the AIS category do present with characteristic syndrome features. So, what is the AIS syndrome?
The Adolescent Idiopathic Scoliosis (AIS) Syndrome
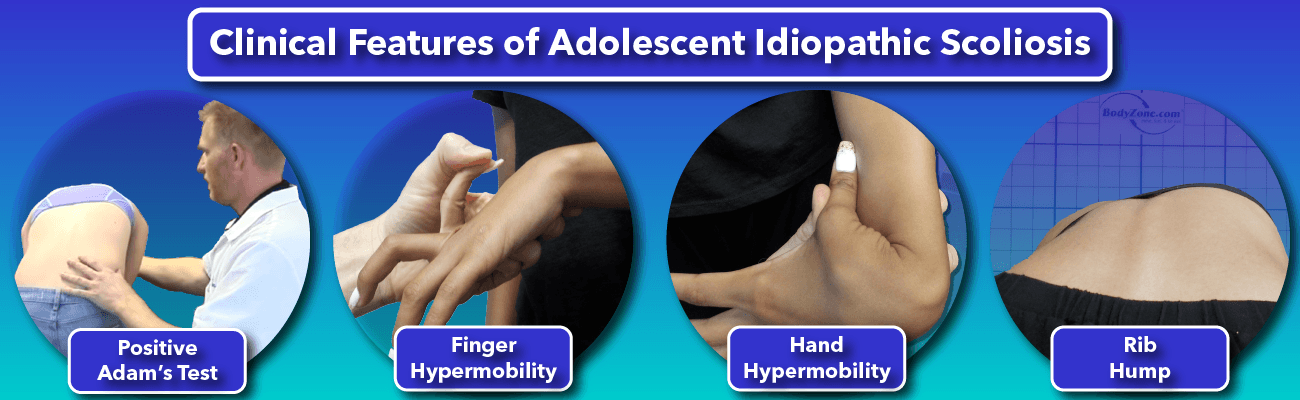
Even though AIS is supposed to simply represent adolescents with scoliosis in which the cause is not yet known, there are many characteristic “syndrome-like” behaviors of curves in this diagnostic category. Below are some of the key clinical features of AIS:
Scoliosis is a Three-Dimensional Problem
AIS is a true Three-dimensional scoliosis, having both a bend and twist of the spine, in contrast to postural deformities which have no twisting. Such postural deformities, or “pseudo-scoliosis” cases, are not progressive and may occasionally respond well to traditional physical therapy or chiropractic intervention. This is not the case with “true” Adolescent Idiopathic Scoliosis. Confusion over what is a true scoliosis and what is a “pseudo-scoliosis” has led some chiropractors and therapists to erroneously conclude that they can treat or cure scoliosis.2
Adolescent Idiopathic Scoliosis Often is Said to Have “No Identifiable Cause”
In the traditional medical model, this means that obvious causes of scoliosis have been ruled out. This means that the adolescent case of scoliosis has:
- No neuromuscular disorders (though mild “sub-clinical” neuromuscular deficiencies are observed with AIS3,4)
- No congenital anomalies
- No Genetic syndromes such as Marfan’s, Ehlers-Danlos, or any other known syndrome which is associated with scoliosis. AIS cases are otherwise healthy kids, with a progressive scoliosis of unknown cause.
Progresses with growth
Adolescent Idiopathic Scoliosis progresses (worsens) with skeletal growth5,6. The faster a child grows, the faster the curve becomes worse, and this worsening of the curve may continue for months after a growth spurt6. The problem is, that while some AIS cases grow only slightly worse, others can grow severely worse and require highly invasive spinal surgery. Predicting who is at risk for a severe curve is a key priority in the management of AIS.7
Rapid worsening stops with skeletal maturity
As growth slows to a stop, rapid worsening of the scoliosis comes to an end. From that point, as the child enters adulthood, AIS may or may not progress slowly over the decades.8 This may depend on variables such as the size of the curve, the location of the curve, and the postural balance of the spine.
Adam’s Forward Bending Test is positive
The classic screening test for scoliosis, often performed by pediatricians and by school screenings, is the Adam’s Forward Bending Test9. The standing child is instructed to bend forward while the examiner views the back from behind. If a rib hump appears when the child is in the forward bent position, this is considered a positive test. A more sensitive screening can be obtained through the use of a “Scoliometer” to measure the degrees of rib hump.10
Structural Deformity
Characteristic structural changes can take place in both the muscles and bones of the spine. Bear in mind that these changes begin with what is a normal, straight spine, but as the patient grows, the following changes can be observed:
Rib Hump
Often the rib hump is first only observed when performing the Adam’s Forward Bending Test, and it will disappear upon returning to the upright posture. Over time, rib humps transition from being present only when bending forward to being present when standing upright.
Flat Back
A flattening of the thoracic spine’s normal kyphotic curve will often precede any scoliosis bending or twisting. It has been observed to be one of the first structural changes of scoliosis.
How can someone have a rib hump and a flat back?
This may seem contradictory, yet the occurrence of both these phenomenon reveal great insight as to the probable cause of AIS. Both of these changes allow for a shortening of the overall length of the spinal canal, which houses the spinal cord.
The Spinal Cord is the Center of the Twist in Scoliosis
The spine coils-down around the axis of the spinal cord.
Structural changes in the soft tissue and bone
Bones, ligaments, muscles, and discs will change shape to accommodate the coiled-down posture of the spine. This change in shape happens gradually as the curves persist during growth, and can become quite rigid as scoliosis matures.
Skinny, tall and flexible females
AIS tends to be more common in females with low body mass 11 and hyper-mobile joints 12. Female dancers and gymnasts seem to have a higher prevalence of scoliosis as they fit this stereotype. However, there are also a fair share of normal and overweight females of average height with the condition.
A Characteristic Response to Treatment
In general, a true AIS case will have the following responses to treatment:
- AIS is Non-responsive to traditional physical therapy and chiropractic treatment 13.
- Bracing is the only non-surgical treatment shown to significantly reduce the risk of progression in high-risk case types (curves 25 + degrees, skeletally immature)14.
- Scoliosis-specific exercises may help, though not without being used in combination with a brace.
- Surgery is the primary treatment option if curve exceeds (or threatens to exceed) 40-50 degrees.
- The belief among many doctors that AIS can only be helped by surgery is so strong, that if a case happens to improve with non-surgical treatment, it will often be concluded that, “It must not have been Idiopathic Scoliosis.” (Not that this is very scientific!)
It is possible to effectively treat AIS without surgery, as well-designed clinical studies have revealed.14–20
A Tight Spinal Cord
Most AIS cases have a short, tight neural tissue within the spinal canal, such as a tight spinal cord or cauda equina. When surgically correcting Adolescent Idiopathic Scoliosis, the short, tight spinal cord is what limits how straight the spine can be made. The surgeon can remove all other hindrances to a straight spine, cutting out bone and soft-tissue contractures that bind the spine, however, one should not cut the tight spinal cord, for obvious reasons.
When a scoliosis is straightened, the canal that the spinal cord lies within becomes longer (taller), leading to a tensile stretch of the spinal cord. The straighter the surgeon makes the spine, the more tension this can place on the cord. Surgical straighten can pull the cord so tight as to cause paralysis. For this and other reasons, it is now standard procedure to monitor the status of the spinal cord so that over-straighten complications are avoided.21,22
The bottom line is, a common feature of AIS syndrome is a tight spinal cord. It has been hypothesized that this tight spinal cord may be the cause of most cases.23–27
What Causes Adolescent Idiopathic Scoliosis?
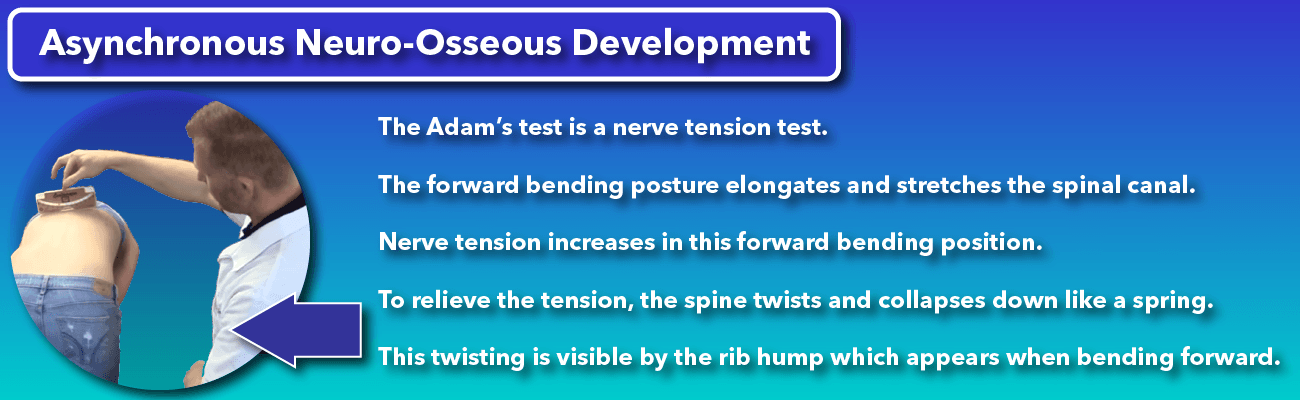
All the structural changes that take place as a normal spine transitions into AIS can be explained by a tight spinal cord. More accurately, tension anywhere along the spinal canal, also called the neural axis, can explain all the changes we see in the alignment of the spine. The official name for this hypothesis first put forward by Dr. Roth is “Asynchronous Neuro-Osseous Development“28,29. The theory states that as the child’s bones grow rapidly, the nervous system or spinal cord is unable to keep up the pace. This results in tension along the axis of the spinal canal, which is relieved by the scoliotic posture.
The mere fact that surgeons are limited by this tightness should be a big hint as to the significance of the tight spinal cord observation. Here are some of the key structural findings of AIS that are 100% explained by tension along the spinal canal:
The Adam’s test is a nerve tension test
The scoliosis screening test known as Adam’s forward bending test, is a nerve tension test. The forward bending posture of Adam’s test results in an elongation and stretch of the spinal canal. Nerve tension increases in this forward bent position, and to relieve that tension the spine twists and collapses down like a spring. This twisting is evidenced by the rib hump which appears when the child bends forward.
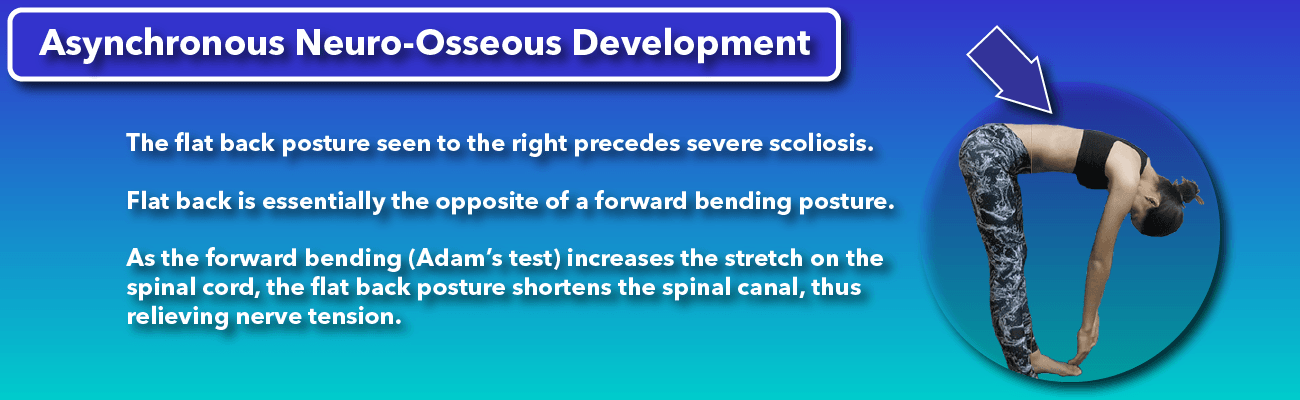
“Flat Back” relieves the tight spinal cord tension
The Flat Back posture which precedes the onset of severe scoliosis is explained by nerve tension. Flat back posture is simply the opposite of the forward bent posture. Since the Adam’s forward bending Test increases stretch on the spinal cord, the flat back posture shortens the spinal canal, relieving nerve tension.
Worsening with growth
Asynchronous growth between the spinal cord and the bones. It is common sense that during growth spurts the bones are growing tall at a fast rate. If the spinal cord is unable to keep up with this growth, a continual increase in nerve tension will occur. More rapid growth means a more rapid increase in nerve tension. Since scoliosis is a posture that shortens the spinal canal and relieves nerve tension, rapid growth results in rapid worsening and collapse of the scoliosis.
Scoliosis itself is a posture that shortens the spinal canal, relieving nerve tension.
“Adolescent Idiopathic Scoliosis” should be a term reserved for a scoliosis curve that is still awaiting a diagnosis. Clearly, it is not being used that way. Rather, the term is being used as a diagnosis of a syndrome with the above features. A preponderance of evidence points to a tight spinal cord as a probable cause for many cases.
So, if you or your child are told they have Adolescent Idiopathic Scoliosis, remember this: It happens for a reason, its causes are knowable, and the condition can be successfully treated without surgery. For more information on how AIS can be treated successfully without surgery, you can read our page regarding treating children and teens for scoliosis; alternatively you can learn more about our comprehensive treatment method, the Silicon Valley Method as well.
References
- Burwell RG, Dangerfield PH, Moulton A, Grivas TB, Cheng JC. Whither the etiopathogenesis (and scoliogeny) of adolescent idiopathic scoliosis? Incorporating presentations on scoliogeny at the 2012 IRSSD and SRS meetings. Scoliosis 2013;8:4.
- Byun S, Han D. The effect of chiropractic techniques on the Cobb angle in idiopathic scoliosis arising in adolescence. J Phys Ther Sci 2016;28:1106–10.
- Cakrt O, Slaby K, Viktorinova L, Kolar P, Jerabek J. Subjective visual vertical in patients with idiopatic scoliosis. J Vestib Res 2011;21:161–5.
- Antoniadou N, Hatzitaki V, Stavridis SΙ, Samoladas E. Verticality perception reveals a vestibular deficit in adolescents with idiopathic scoliosis. Exp Brain Res 2018.
- Ylikoski M. Growth and progression of adolescent idiopathic scoliosis in girls. J Pediatr Orthop B 2005;14:320–4.
- Cheung JPY, Cheung PWH, Samartzis D, Luk KD-K. Curve Progression in Adolescent Idiopathic Scoliosis Does Not Match Skeletal Growth. Clinical Orthopaedics and Related Research 2018;476:429–36.
- Dimeglio A, Canavese F. Progression or not progression? How to deal with adolescent idiopathic scoliosis during puberty. J Child Orthop 2013;7:43–9.
- Agabegi SS, Kazemi N, Sturm PF, Mehlman CT. Natural History of Adolescent Idiopathic Scoliosis in Skeletally Mature Patients: A Critical Review. J Am Acad Orthop Surg 2015;23:714–23.
- Bunnell WP. An objective criterion for scoliosis screening. J Bone Joint Surg Am 1984;66:1381–7.
- Coelho DM, Bonagamba GH, Oliveira AS. Scoliometer measurements of patients with idiopathic scoliosis. Braz J Phys Ther 2013;17:179–84.
- Liu Z, Tam EMS, Sun G-Q, et al. Abnormal leptin bioavailability in adolescent idiopathic scoliosis: an important new finding. Spine (Phila Pa 1976) 2012;37:599–604.
- Arponen H, Mäkitie O, Waltimo-Sirén J. Association between joint hypermobility, scoliosis, and cranial base anomalies in paediatric Osteogenesis imperfecta patients: a retrospective cross-sectional study. BMC Musculoskelet Disord 2014;15.
- Lantz CA, Chen J. Effect of chiropractic intervention on small scoliotic curves in younger subjects: a time-series cohort design. J Manipulative Physiol Ther 2001;24:385–93.
- Weinstein SL, Dolan LA, Wright JG, Dobbs MB. Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med 2013;369:1512–21.
- Aulisa AG, Guzzanti V, Falciglia F, Galli M, Pizzetti P, Aulisa L. Curve progression after long-term brace treatment in adolescent idiopathic scoliosis, Comparative results between over and under 30 Cobb degrees – SOSORT 2017 award winner. Scoliosis Spinal Disord 2017;12:36.
- Bettany-Saltikov J, Turnbull D, Ng SY, Webb R. Management of Spinal Deformities and Evidence of Treatment Effectiveness. Open Orthop J 2017;11:1521–47.
- Kwan KYH, Cheng ACS, Koh HY, Chiu AYY, Cheung KMC. Effectiveness of Schroth exercises during bracing in adolescent idiopathic scoliosis, Results from a preliminary study-SOSORT Award 2017 Winner. Scoliosis Spinal Disord 2017;12:32.
- Moramarco M, Moramarco K, Fadzan M. Cobb Angle Reduction in a Nearly Skeletally Mature Adolescent (Risser 4) After Pattern-Specific Scoliosis Rehabilitation (PSSR). Open Orthop J 2017;11:1490–9.
- Shokei Yamada, MD, PhD, FACS. Tethered Cord Syndrome. https://rarediseases.org/rare-diseases/tethered-cord-syndrome/.
- Romano M, Negrini A, Parzini S, et al. SEAS (Scientific Exercises Approach to Scoliosis): a modern and effective evidence based approach to physiotherapic specific scoliosis exercises. Scoliosis 2015;10.
- Pastorelli F, Di Silvestre M, Plasmati R, et al. The prevention of neural complications in the surgical treatment of scoliosis: the role of the neurophysiological intraoperative monitoring. Eur Spine J 2011;20 Suppl 1:S105-14.
- Mineiro J, Weinstein SL. Delayed postoperative paraparesis in scoliosis surgery. A case report. Spine (Phila Pa 1976) 1997;22:1668–72.
- Chu WC, Lam WM, Ng BK, et al. Relative shortening and functional tethering of spinal cord in adolescent scoliosis – Result of asynchronous neuro-osseous growth, summary of an electronic focus group debate of the IBSE. Scoliosis 2008;3:8.
- Chu WCW, Deng M, Hui SCN, et al. Spinal cord morphology predicts curve progression in adolescent idiopathic scoliosis treated with bracing?, A prospective cohort study with magnetic resonance imaging. Scoliosis 2015;10.
- Porter RW. The pathogenesis of idiopathic scoliosis: uncoupled neuro-osseous growth?, Uncoupled neuro-osseous growth? Eur Spine J 2001;10:473–81.
- Porter RW. Can a short spinal cord produce scoliosis? Eur Spine J 2001;10:2–9.
- Roth M. Idiopathic scoliosis caused by a short spinal cord. Acta Radiol Diagn (Stockh) 1968;7:257–71.
- Roth M. Neurovertebral and Osteoneural Growth Relations, A concept of normal and pathological development of the skeleton. Univerzita J.E. Purkyne, Brno: Radiodiagnositic Clinic, Medical Faculty, 1985. 101 p.
- Roth M. Idiopathic scoliosis from the point of view of the neuroradiologist. Neuroradiology 1981;21:133–8.