Scoliosis Progression: Why it Worsens with Growth
For children with adolescent idiopathic scoliosis, both parents and kids with a curve will worry whether or not the curve will get larger and worsen over time. Worrying about a curve progressing is completely understandable as many curves rapidly get worse as a child grows, especially once they hit puberty. But why does a scoliosis get worse with growth? What is it about puberty and a child growing that causes a curve to get bigger? This article will talk about why a scoliosis gets worse with growth and what can be done to prevent this from happening.
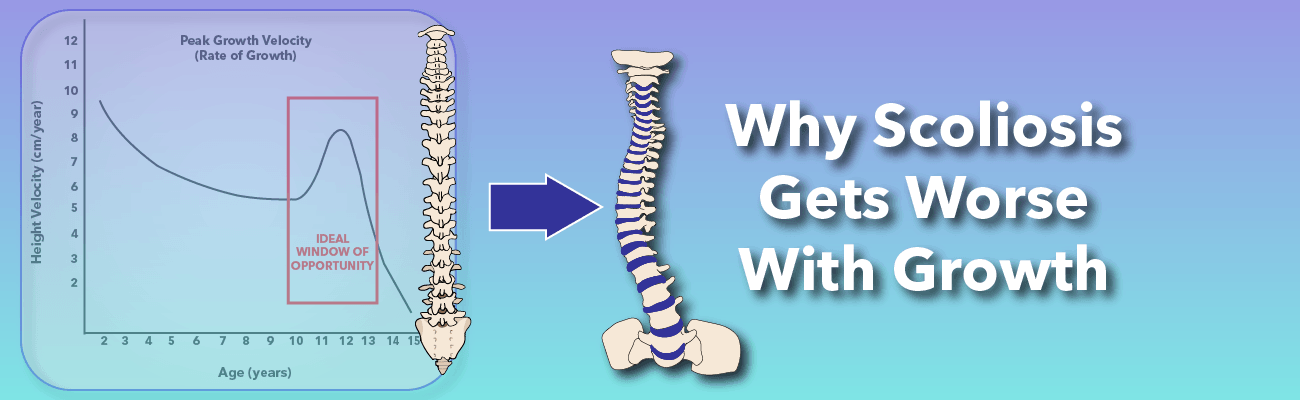
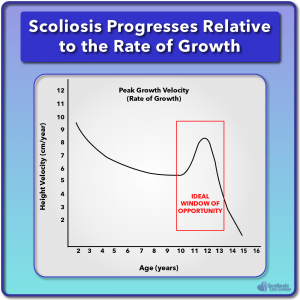
For kids with idiopathic scoliosis, research has shown that the average age when a scoliosis will begin to get rapidly worse is about 11 to 12 years old 1. However, we also know from research that when a scoliosis develops and starts to progress is actually related to HOW FAST we grow, and how much growing we still have left to do2.
This “timing” of growth is related to when we start and finish puberty and while when puberty starts can’t be easily predicted, how far along a child is in puberty can be estimated by looking at their BONE AGE (skeletal maturity) rather than their chronological age (how old they are)3. This is because a child or teen’s bone age reflects how much growth they have left; how much more they will grow before they reach skeletal maturity.
How fast a child grows and how much growing they have left to do is critical to whether a curve will get worse or not
As you would imagine, this depends on how far along through puberty they are and whether they have hit their growth spurt during puberty. This growth spurt that happens to all of us as we go through puberty is known as the adolescent growth spurt and is directly related to scoliosis and when it becomes a problem as the curve rapidly grows in size.
Where Does Scoliosis Come From?
While a curve may seem to get worse almost overnight, with curves sometimes doubling in size in a short (6 month) period of time 4, scoliosis does not magically appear; it develops over time. While some types of scoliosis (neuromuscular, congenital, and syndromic) can be related to other underlying problems such as a tethered cord or Marfan’s syndrome, idiopathic is more often than not said to have no known cause; hence the term idiopathic. However over the past 60 years more and more evidence has been found suggesting that idiopathic scoliosis may come from an underlying problem with the nerves and spinal cord: nerve tension.
Nerve tension was first proposed as the cause of idiopathic scoliosis in the 1960’s
The idea that a tight or short spinal cord and nerve tension could be the driving force or root cause behind idiopathic scoliosis is nothing new. As we have mentioned in other articles, Dr. Milan Roth first discussed the idea of a tight spinal cord being the root cause of idiopathic scoliosis in the 1960’s. Then in the late 90’s and early 2000’s, a spinal surgeon by the name of Dr. Richard Porter rediscovered Dr. Roth’s research and studied the idea more. Then in the early 2010’s, with the use of modern medical technologies such as the MRI, Dr. Chu performed more research investigating scoliosis and how it can be caused by tight nerves. Over all those years each doctor made similar observations and came to the same conclusion: a tight spinal cord or tight nerves cause the spine to adapt and begins the process of a scoliosis curve developing.
When Does Scoliosis Appear? When Does It Begin?
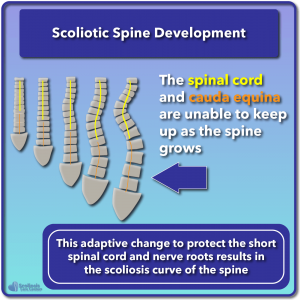
If you have read our article on nerve tension and how it relates to scoliosis, you will learn in detail about how tight nerves and a tight spinal cord can cause the sideways curve and rotation of the vertebrae we see in scoliosis. We will talk about a lot of this in a moment, but in summary a scoliosis will begin to develop and a curve will start to appear as the spine tries to adapt to the tight spinal cord and nerves in an effort to relieve tension. Just as a guitar string is pulled tight, the spinal cord can be pulled tight because of the spine growing FASTER than the spinal cord.
If the nerves and spinal cord can’t keep up with how fast the bones of the spine are growing nerve tension will occur
As the spinal cord is left in the dust behind the rapidly growing vertebrae and spinal column, the cord is pulled tight and as a result the body tries to find a way to release this tension. The more the spinal bones grow, the shorter the spinal cord, and the tighter the nerves are, the more the body needs to change to adapt to this tension. Unfortunately these tension relieving adaptations result in more and more scoliotic deformities, beginning with a flat back, progressing to a sideways bend or curve, and then eventually requiring the vertebrae to rotate as well to release the tension and provide the spinal cord with the shortest path possible. We will go into more detail about this in a minute after we quickly talk about when scoliosis stops progressing.
When Does Scoliosis Stop Getting Worse?
If the spine is growing faster than the spinal cord and nerves can keep up with, and if the body is doing its best to adapt to the nerve tension that occurs because of this spine versus nerve “race”, and if these adaptations are the rotation and curve we see in scoliosis, when will the scoliosis stop getting worse? When will the curve stop growing?
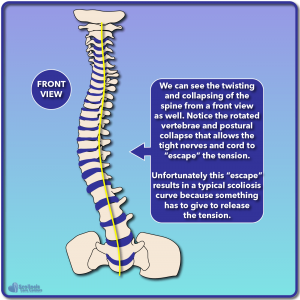
The spine will buckle into a curve and rotate in an effort to relieve nerve tension
As you might imagine, the scoliosis will stop getting worse once there is no longer any additional tension to relieve. For this to happen, the spine needs to stop growing and for the spine to stop growing we need to reach skeletal maturity. Once the body has reached skeletal maturity at the end of puberty, we have reached our adult height and while some bones may continue to grow to some extent (ie. the pelvis) the spine has completed its growth. Because the spine has finished growing, the nerves and spinal cord no longer need to attempt to catch up, and the curve will stop progressing. It’s important to note that we are talking about RAPID progression after skeletal maturity of the curve and not a slow worsening with age as we observe in some adults with untreated scoliosis (mostly in curves >30º)5 and even in people who have had scoliosis surgery (spinal fusion)6.
Why How Fast We Grow (Rate Of Growth) Is Critical To Scoliosis
After we are born, the body grows very rapidly during our early childhood years (to about age 3) and then slows down until we hit the adolescent growth spurt. During this time, we grow faster than any other time in our life other than early childhood; another way of saying this is that our rate of growth is highest during the adolescent growth spurt (aside from early childhood). During this rapid period of growth the spine can quickly outpace the spinal cord resulting in additional nerve tension. As nerve tension increases, the body needs to adapt even more resulting in the tell-tale scoliosis deformities (curve, rotation) that we discussed earlier.
Research Shows Kids With Scoliosis Have Longer Spines With Changes In Shape
Let’s get a little bit technical for a moment. If we look at any given vertebrae in the spine, we see that the biggest part is called the vertebral body, with two smaller parts known as pedicles connecting the body to the other parts of the vertebrae (the lamina, transverse, and spinus process). We see a hole in the back of the spine(known as the central canal) where the spinal canal is located and within the spinal canal we will find the spinal cord. Ultimately, the spinal cord has a big influence on whether or not the canal develops correctly. If the spinal cord does not grow at the same speed as the bones of the spine, the cord will try to stay in the center as much as it can while the vertebral bodies will begin to deform and buckle over time.7,8
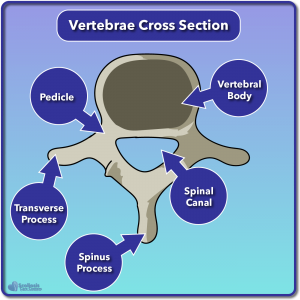
The spinal cord influences how the spine develops
These deformities as well as the spine growing faster than the spinal cord/nerves have actually been reported in scientific and medical studies. Girls with adolescent idiopathic scoliosis had taller vertebral bodies and shorter pedicles compared to girls without scoliosis9. In fact the vertebral bodies were found to grow longer in girls with idiopathic scoliosis than those without scoliosis9. This same observation was made by a different study that not only found people with adolescent idiopathic scoliosis had a longer vertebral column, but that their spinal cord length was not proportionately as long as it should be compared to people without scoliosis. Additionally, they saw the spinal cord was consistently off to one side of the spinal column, more on the concave side of the scoliosis curve.10
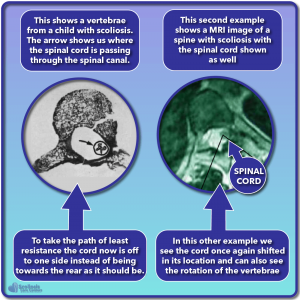
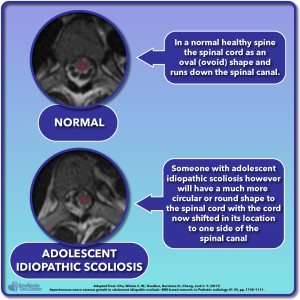
The spinal cord shifting off to one side, specifically the concave side of the curve has been observed many times by scientists and doctors11,12. What is equally fascinating is that when seen using MRI, the spinal cord was in fact shorter than it should be relative to the length of the spine especially in the case of LARGE scoliosis curves12. The MRI imaging also showed the cord’s shape had changed: instead of the usual oval shape it was now more round and smaller in diameter12. This makes sense because if nerve tension was present, we would expect changes in shape and the cord to shift its position.12
The spine will grow longer and faster than the spinal cord in idiopathic scoliosis
When The Spine Grows Faster Than The Spinal Cord
With evidence that the spinal cord is tight and shorter than it should be (ie. change in shape and location and MRI imaging) while the spine and its vertebral bodies continue to grow at a fast pace, it is likely that these two things are related9. A spine growing faster than the spinal cord can keep up with is referred to by scientists as uncoupled or asynchronous neuro-osseous growth: uncoupled/asynchronous meaning they don’t grow at the same pace; neuro meaning nerves and the nervous system and spinal cord; and osseous referring to bones of the spine.
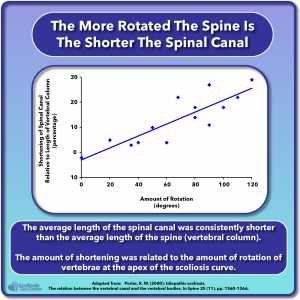
He observed that the spinal canal was on average 14% shorter than it should have been, but ALSO noticed that how short it was is related to the size of the scoliosis curve, but even more so was related to how much rotation had occurred7. Keeping in mind that there was no significant different between the spinal canal length and the spine in people without scoliosis7 this all makes complete sense in relation to nerve tension. The shorter the canal, the shorter the cord, the tighter the nerves; the tighter the nerves, the more the spine needs to adapt and the bigger the curve and the more rotation we see.
Three Steps To Scoliosis: Flat Back, Curve, and Rotation
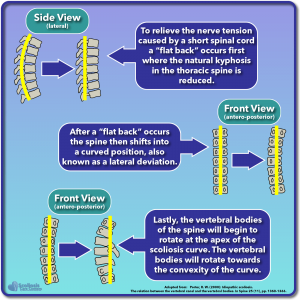
One early warning sign of scoliosis is a “flat back” where the spine loses its normal forward curve (kyphosis) when bending over. In the 1950’s a researcher by the name of Somerville found that in the early stages of scoliosis, a “flat back” occurred followed by a sideways shift (a curve) and then rotation. What is interesting is that Somerville also found that causing tension via tethering caused these deformities to appear15. These observations once again match up with the idea that a tight spinal cord is the root cause behind idiopathic scoliosis as we see a three step process happening as the body tries to relieve the nerve tension that results from a tight spinal cord7.
First, we see the natural kyphosis disappear as a result of the tight spinal cord. Then, we see the cord shift to one side of the spinal canal (the concave side of the curve) in an effort to take the shortest path possible. This shift in position causes the spine to bend to one side: the hallmark scoliosis curve. Lastly we see the spine buckle and rotate again in an effort to provide the shortest path possible for the tight spinal cord7. We find even more evidence supporting this idea as the biggest deformities occur close to the apex of the scoliosis curve, while a torsion (a rotational force) was observed which is likely the short/tight spinal cord16. All of this research combined provides a lot of evidence that our smoking gun behind idiopathic scoliosis is nerve tension that results from uneven growth of the spinal cord relative to the spine: asynchronous neuro-osseous development
Why Scoliosis Progresses With Growth
Let’s quickly recap what we have learned and then tie it all together with growth and a child’s adolescent growth spurts. Kids without scoliosis have a spinal cord that is not significantly shorter than their spine (vertebral column) while kids with adolescent idiopathic scoliosis can have significantly shorter spinal cords relative to their spine. When the spinal cord is short, it still needs to span the length of the spine and as a result it changes in shape as it stretches. The body then adapts to this nerve tension by trying to provide the tight spinal cord with the shortest path possible. To do this, the spine buckles, a curve forms, and rotation occurs resulting in a typical scoliosis.
If we stretch the spinal cord and relieve the nerve tension we can help prevent the spine from buckling, curving and rotating
We know from science and medical research that scoliosis progression is associated with the adolescent growth spurt when the body rapidly grows13, 17–21 and that after puberty begins, kids with scoliosis are taller than those who don’t have a curve. These differences in height got progressively bigger as they progressed through puberty22. Additionally, girls with scoliosis have an abnormally faster RATE OF GROWTH compared to those who don’t22.
While THE AMOUNT of nerve tension present will vary from scoliosis to scoliosis, if the spinal cord is not growing as fast as it should the nerve tension WILL INCREASE during the adolescent growth spurt and the scoliosis WILL WORSEN as the body tries to adapt and relieve the tension. Dr Roth’s research, Dr. Porter’s, Dr. Chu’s, and other researchers’ observations and data all point to this nerve tension problem driving the development of a curve and rotation.
Closing Remarks
If we can safely and slowly stretch the tight spinal cord and nerves, then we can effectively reduce nerve tension. If we reduce the tension, the spine no longer needs to rotate, buckle and collapse in order to release tension. If we then help straighten the spine and hold it there until the spine has finished growing, we now have not only taken care of the root cause of the scoliosis curve, but have also reduced the curve and used the adolescent growth spurt to our advantage to straighten the spine.
While the idea that nerve tension causing scoliosis may have started in the 1960’s, with the help of modern hyper-correct bracing and MRI imaging how we understand and treat a curve is now drastically improved compared to just a decade ago.
References
- Sanders, J. O. et al. Maturity assessment and curve progression in girls with idiopathic scoliosis. The Journal of bone and joint surgery. American volume 89, 64–73 (2007).
- Ylikoski, M. Growth and progression of adolescent idiopathic scoliosis in girls. Journal of pediatric orthopedics. Part B 14, 320–324 (2005).
- Melmed, S., Polonsky, K. S., Larsen, P. R. & Kronenberg, H. Williams textbook of endocrinology (Elsevier, Philadelphia, PA, 2016).
- Dimeglio, A. & Canavese, F. Progression or not progression? How to deal with adolescent idiopathic scoliosis during puberty. Journal of children’s orthopaedics 7, 43–49 (2013).
- Weinstein, S. L. The Natural History of Adolescent Idiopathic Scoliosis. Journal of pediatric orthopedics 39, S44-S46 (2019).
- Danielsson, A. J. & Nachemson, A. L. Radiologic findings and curve progression 22 years after treatment for adolescent idiopathic scoliosis. Spine 26, 516–525 (2001).
- Porter, R. W. Idiopathic scoliosis. The relation between the vertebral canal and the vertebral bodies. Spine 25, 1360–1366 (2000).
- Ursu, T. R., Porter, R. W. & Navaratnam, V. Development of the lumbar and sacral vertebral canal in utero. Spine 21, 2705–2708 (1996).
- Chu, W. C. W., Rasalkar, D. D. & Cheng, J. C. Y. Asynchronous neuro-osseous growth in adolescent idiopathic scoliosis–MRI-based research. Pediatric radiology 41, 1100–1111 (2011).
- Chu, W. C. et al. Relative shortening and functional tethering of spinal cord in adolescent scoliosis. Scoliosis 3, 8 (2008).
- Liljenqvist, U. R. et al. Analysis of vertebral morphology in idiopathic scoliosis. The Journal of bone and joint surgery. American volume 84, 359–368 (2002).
- Chu, W. C. W. et al. Morphological and functional electrophysiological evidence of relative spinal cord tethering. Spine 33, 673–680 (2008).
- Roth, M. Idiopathic scoliosis caused by a short spinal cord. Acta radiologica: diagnosis 7, 257–271 (1968).
- Porter, R. W. The pathogenesis of idiopathic scoliosis: uncoupled neuro-osseous growth? European spine journal 10, 473–481 (2001).
- Somerville, E. W. Rotational lordosis; the development of single curve. The Journal of bone and joint surgery. British volume 34-B, 421–427 (1952).
- Wever, D. J. et al. A biomechanical analysis of the vertebral and rib deformities. Eur Spine J 8, 252–260 (1999).
- Howell, F. R., Mahood, J. K. & Dickson, R. A. Growth beyond skeletal maturity. Spine 17, 437–440 (1992).
- Little, D. G. et al. Relationship of peak height velocity to other maturity indicators. The Journal of bone and joint surgery. American volume 82, 685–693 (2000).
- Nissinen, M. et al. Trunk asymmetry, posture, growth, and risk of scoliosis. Spine 18, 8–13 (1993).
- Shohat, M. et al. Growth and ethnicity in scoliosis. Acta orthopaedica Scandinavica 59, 310–313 (1988).
- Song, K. M. & Little, D. G. Peak height velocity as a maturity indicator. Journal of pediatric orthopedics 20, 286–288 (2000).
- Siu King Cheung, C. et al. Abnormal peri-pubertal anthropometric measurements and growth pattern. Spine 28, 2152–2157 (2003).
- Potenza, V. et al. Dysfunction of the spinal cord during spinal arthrodesis. The Journal of bone and joint surgery. American volume 80, 1679–1683 (1998).
- Floman, Y. Thoracic scoliosis and restricted neck motion. Eur Spine J 7, 155–157 (1998).
- Breig, A. Overstretching of and circumscribed pathological tension in the spinal cord. Journal of biomechanics 3, 7–9 (1970).