Written and reviewed for scientific and factual accuracy by Dr. Austin Jelcick, PhD and Dr. Matthew Janzen, DC. Last reviewed/edited on March 10, 2020. First published October 30, 2019.
“An old man turned ninety-eight, he won the lottery and died the next day.” This may be a lyric from Alanis Morissette’s song Ironic, but think about it in the context of scoliosis bracing: if we wear a brace just for our scoliosis to get worse in the end, what was the point? On the other hand, just like wearing a cast after breaking an arm isn’t the most fun thing in the world, if it lets the arm heal (of in our case if the brace stops the scoliosis), then it was worth it. But will it be worth it? Is bracing for scoliosis effective? Or is bracing just setting us up for an ironic ending?
CLAIM: Scoliosis bracing is not effective for treating scoliosis and cannot stop a curve from worsening or prevent surgery.
EXAMPLE: “Bracing is not proven to stop scoliosis progression or reduce need for surgery.”
ORIGIN: Seen on various scoliosis info pages including ScoliSmart, ScoliosisCorrectionCenters, and various non-surgical clinics as of October 2019.
CONCLUSION: FALSE: Bracing has been shown to be effective at preventing surgery, preventing progression of a curve, and reducing curves when performed correctly.
Am I Being Educated Or Misinformed?
If you do a quick search about scoliosis bracing online, you may find many sensational predatory websites announcing that bracing is outdated; bracing is ineffective and doesn’t work; that bracing doesn’t stop a curve from worsening (progression); and that bracing doesn’t even prevent surgery. While it is true that old research had some debatable evidence supporting bracing being effective, in the last decade multiple ground breaking studies have put this issue to rest. Between properly performed, scientifically sound, randomized clinical trials to retrospective studies, bracing has been proven beyond a shadow of a doubt to be effective at treating idiopathic scoliosis.
There is a lot of misinformation online about bracing that continues to be spread by predatory clinics through sensational and emotional social media posts using “cherry picked” scientific information. This fact check article focuses on the large body of scientific evidence that shows bracing for scoliosis is effective and can stop progression, prevent surgery, and even reduce curves.
The effectiveness of bracing used to be debated, but current research has proven scoliosis bracing to work
While it is true that older research had some debatable evidence supporting bracing being effective, in the last decade multiple ground breaking studies have put this issue to rest. Between properly performed, scientifically sound, randomized clinical trials to retrospective studies, bracing has been proven beyond a shadow of a doubt to be effective at treating scoliosis.
Last Century’s Research Was Inconclusive
Just because research is old doesn’t necessarily mean it is no longer relevant. However, when looking at old versus new research we need to understand and look for key differences that could significantly impact the results. For bracing, one of the BIGGEST things that has changed over the years (a variable in scientific language) is the brace itself. Scoliosis bracing has come a long way over the last 50 years, evolving from hard casts to highly customized hyper-corrective braces that are designed with the assistance of a computer. As you would imagine, as braces evolved over time their purpose did as well: shifting from simply trying to hold the spine in place to prevent worsening to actually straightening the spine. We will discuss why this is important later on but for now just know that straightening the spine in the brace is important.
Even though some older studies did not find bracing to be effective, there are still some older studies that support bracing, hence why “the jury was still out” with regards to bracing until the last decade or so. One such study looked at people who treated their scoliosis in the 1960’s and 1970’s, either using bracing or undergoing surgery, receiving Herrington rods to straighten their scoliosis. The study followed these people for 20 years after they finished treatment and looked to see which group did better at preventing progression (worsening) of their curves. Despite the in-brace correction provided by these old brace designs, they found that in most cases, neither group’s curves increased in size 20 years after treatment. 1
Bracing is the only non-surgical treatment proved to prevent surgery and stop a curve from worsening
Over the years several other studies asked the question if bracing was effective, using a variety of different brace types and designs. In addition to varying designs, how the braces were used varied. Some looked at full time brace wear while others looked at part time brace wear. Some focused on full-time braces that are widely prescribed such as the Boston brace 2, while others focused only on night time braces 3. Despite all of these variables and differences between how bracing was used, each study found bracing to be effective at treating scoliosis. The overall consensus or take home message from all of these studies combined is simply that for children who are still growing (skeletally immature) and have idiopathic scoliosis, bracing is the only treatment proven to be effective at limiting progression and preventing surgery. 4, 5, 6, 7
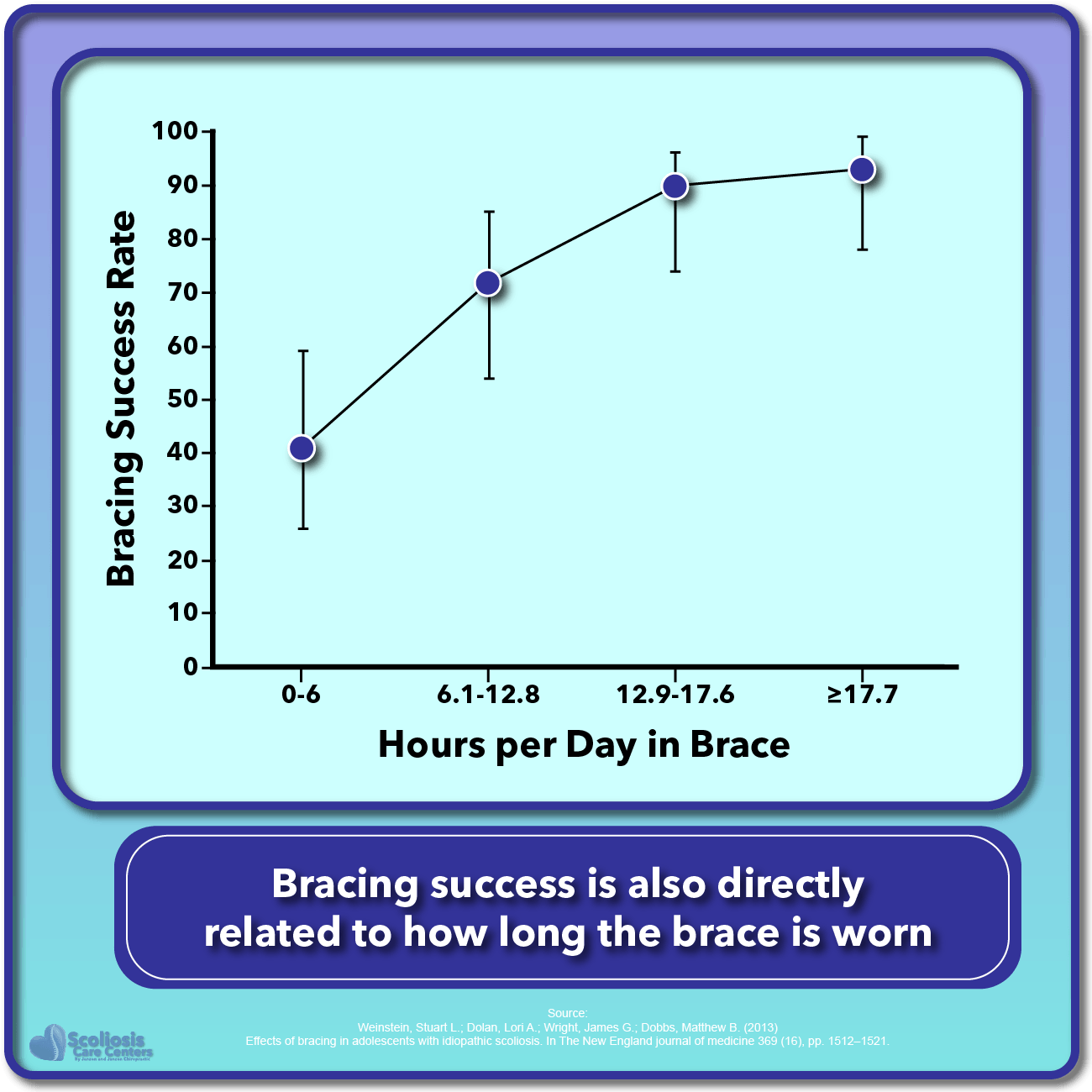
As bracing improved and more research was done, some interesting observations were made. These observations would eventually develop into trends and then eventually into treatment guidelines for bracing; specifically regarding how long a brace should be worn for it to be effective. One such study from the mid 1990’s made the observation that when the brace was worn 23 hours of the day progression of the scoliosis was stopped. However, when brace wear decreased to only 16 hours or less, the effectiveness of the brace was SIGNIFICANTLY lower. 8

This simple concept that “the more you wear the brace the more effective it is” is repeated in research and clinical studies, and we will come back to it again when we talk about current research in a bit. But it is critical to understand this seemingly obvious concept: for a brace to be effective it needs to be worn as close to 24 hours a day as possible. After all the brace is trying to keep the spine straight as it grows, and growth doesn’t stop when you sleep or take lunch breaks.
The simple idea that “the more you wear the brace the more effective it is” is repeatedly proven in research and clinical studies
As time went on and we entered the 2000’s, major improvements occurred in the world of scoliosis bracing. Computer aided designs as well as new research finding key factors that influence how successful a brace is at straightening the spine began to emerge. As bracing improved, clunky casts and cookie cutter braces began to evolve into custom fit hyper-corrective braces that were designed for an individual patient’s curve, spine, and body. These improvements and changes were not simply “shots in the dark” or new ways to jazz up a brace to make kids want to wear them more. These improvements affected how straight the brace could make the spine and how long the patient could wear the brace comfortably; two key factors that we will talk about next.
In 2003 research came out saying that if in-brace correction was less than 20% that bracing wasn’t a good idea 9. What this essentially says is that if a curve isn’t improved by at least 20% while wearing the brace, such as a 35º curve reducing down to 28º, then a brace wasn’t worthwhile. Because a child is still growing we can use their growth spurts to our advantage in guiding the spine straight before the child becomes skeletally mature. Thus, how straight we make the spine in the brace is the basis for what the spine will be like when treatment is finished. So if we aren’t correcting it that much then what is the point of the brace other than to try and hold it in place, despite the fact that some older studies found this to not be effective?
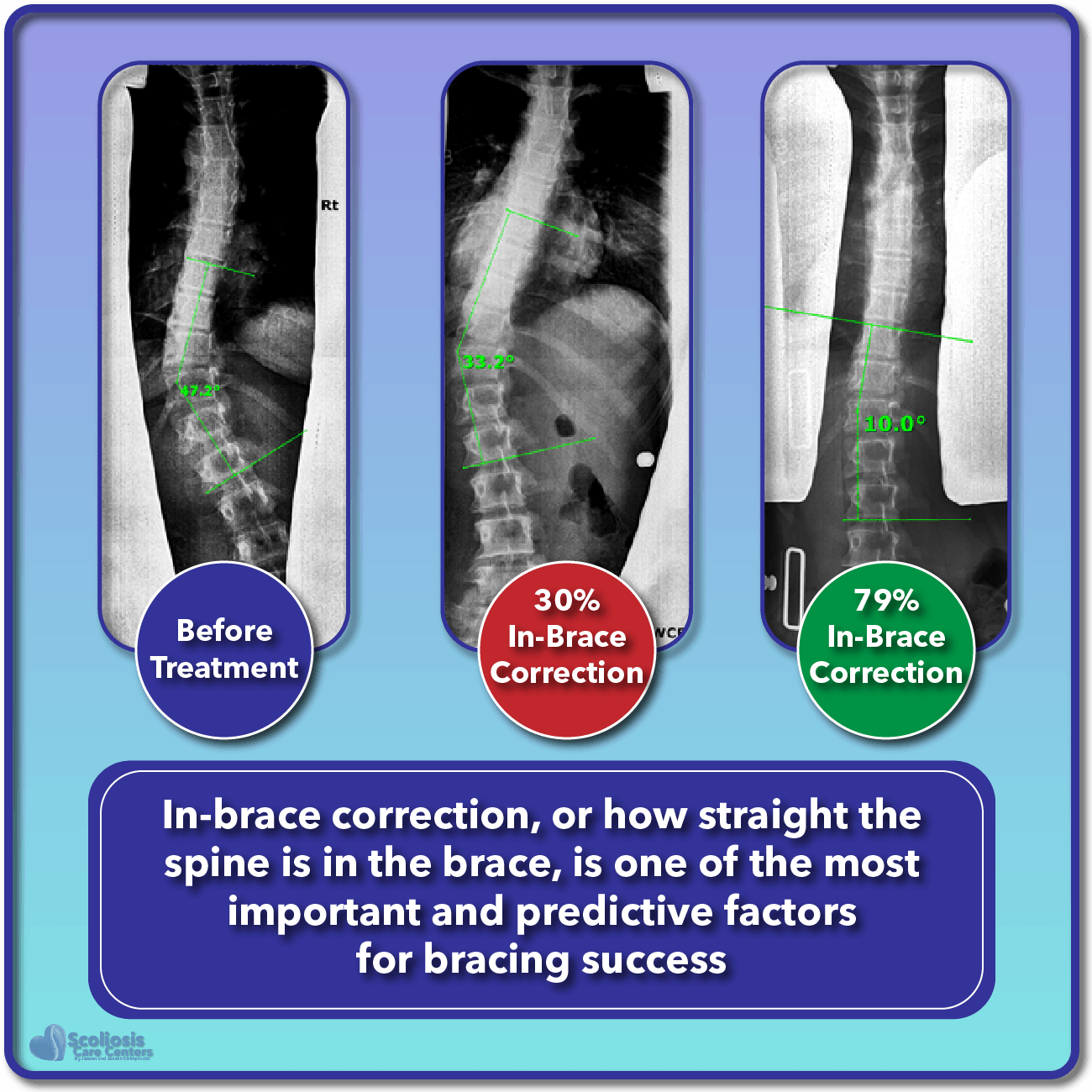
Success Is Directly Related To How Straight The Spine Is In The Brace
The idea that making the spine straight in-brace is a helpful predictor about treatment success seems somewhat obvious, but the fact is it has been researched extensively. While the amount of in-brace correction needed for the best treatment outcome is debated, ranging from 25% 10 to 40% or more 11, there is a solid body of research that shows that how straight we make the spine while wearing the brace significantly impacts the outcome of treatment and is a good predictor of how much we can correct a curve 12.
Going back to one of our first points that wearing the brace as much as possible is important, a much older study from 1986 was ahead of its time as it also found that in-brace correction was important, but that compliant patients (those who wore their brace as prescribed) were more successful in treating their scoliosis than those who were not. With good in-brace correction and good compliance, ~88% were successful versus ~43% who were not as complaint 13. One study we frequently talk about that focuses on the topic of in-brace correction is the 2010 study that again found that in-brace correction was directly related to the long-term outcome of treatment (how successful it was). The added bonus to this study and its findings was that this golden rule of in-brace correction applied to both stiff curves as well as flexible curves. 14
1. How straight the spine is made in the brace and 2. How much the brace is worn is CRITICAL for success
This widely applicable rule that in-brace correction can help both stiff and flexible curves is also important because how stiff a curve is, including its shape, location, and other factors that relate to the TYPE of curve the patient has all influence how well it can be treated 15. However, regardless of curve type, increasing compliance (brace wear) improves treatment outcomes 15. So again we are told by multiple studies that wearing your brace and straightening the curve in the brace are important. Considering some information online tries to say that stiff curves can’t be helped with bracing, it is research like this that helps to dispel the myths and misinformation that exist and show once again that bracing for scoliosis is in fact effective.
Research Shows Time and Time Again That Bracing Is Effective
Before we jump into a laundry list of research that shows bracing to be effective at reducing a scoliosis curve, let’s quickly tackle the emotional question that many predatory clinics talk about: quality of life during bracing. Wearing a brace 23 hours a day is no cake walk, but it also isn’t the same as it used to be with large unsightly metal braces from the turn of the century. With modern lightweight, low profile customized braces, patients can easily “embrace the brace” and make it into both a fashion statement as well as bringing awareness to their peers. They can be covered by clothing easily, and with modified designs available for sporting events and social gatherings, wearing a brace is not the “social doom” many make it out to be. Looking at everything from pain, to bodily function, mental health, and self-image, a 2015 study found that quality of life was similar to the general population 16. This combined with the fact that no progression of the curve was detected 25 years after treatment ended 16 gives us yet another piece of evidence that bracing is not the enemy some clinics make it to be.
When we dive head first into the scientific literature and start looking at all the recent research on bracing, we find suggestions on how to improve bracing, how to improve compliance, and what should be studied next, but we do not find some “smoking gun” saying that bracing is outdated and ineffective. What WE DO FIND is time and time again, research has found that bracing is proven to be effective at reducing the need for surgery, and can improve the external appearance (aka aesthetics) such as posture and rib hump 17. We find research that shows that not only can progression be stopped, but that curves can be significantly improved 18. While the success rates vary, with some reporting success of more than 90% 19, while other report success of ~75% 20, the amount of evidence that shows bracing is effective at stopping a curve from worsening is overwhelming. 21
Research shows repeatedly that bracing is effective at preventing surgery
Recent research using new and improved brace designs and combined treatment programs have again shown that progression of a scoliosis can be stopped, but that this can be achieved with little impact to the lungs and lung capacity 22. The idea that bracing can be effective without affecting the lungs (and vital capacity) is important because once again misinformation abounds online, referencing old studies and playing on fear in an attempt to sway patients away from bracing out of fear their lung capacity will be affected. Considering additional research has shown that the effects of bracing can be improved even more when scoliosis specific exercises (PSSE) are added to a treatment program 23 (exercises in addition to bracing 24, between modern brace designs and physiotherapeutic exercises any impact of the lungs can be easily addressed.
Improving Bracing Research and Long Term Success
We’ve talked about how bracing was controversial at one point until high quality scientific research was performed showing that bracing can prevent surgery and stop progression. We also have briefly talked about how adding specific physiotherapeutic exercises can improve treatment even more, and how wearing a brace as close to 24 hours a day as possible is the best choice 24. While we have talked about how some older studies may provide less than ideal evidence in support of bracing due to the design of the study, the brace, or other variables 24, there have been extremely valuable scientifically rigorous studies performed that cast away any doubt about bracing effectiveness.
A study once said that to save one child from surgery, we would need to treat three 25. However, as bracing has evolved and studies begin to achieve more than 75% success 26, the key ingredients to effective bracing have emerged. How long the brace is worn, patient compliance, and immediate in-brace correction have been shown over and over to be crucial for success 26. With in-brace correction becoming the most important and predictive factor for bracing success 24, we also find that a slow and gradual weaning off the brace AFTER skeletal maturity has been reached can provide success rates of more than 98% 27.
Braces should be worn until skeletal maturity and then slowly weaned off
To truly change the way bracing is understood and stop the misinformation, we need to be even more thorough in how we research bracing. You may have seen countless before and after treatment photos from various clinics showing successful treatment. However many beg the question whether or not the results will last, with photos showing results right after the brace was removed. Short term results of only one or two months are virtually useless in terms of reaching solid reliable conclusions. Even for a treatment that takes 12 months, we need to see results at the end of growth, and possibly even later on well into the patient’s adult years 28. Without these long term studies, good research will continue to be overlooked while low quality research will pull the public away from real science and allow misinformation to persist. 28
Thankfully, there has been some amazing research done that is completely objective and avoids any possible bias or cherry picking of data. We mention the 2013 study by Weinstein quite often, and for good reason. The reason this study is so important is that it followed the scientific approach of “random controls” and blinding. What this means is that when investigating whether bracing is effective, we don’t know what treatment someone gets until AFTER we perform the analysis. This prevents us from skewing the data by interpreting it with rose colored glasses, and it prevents us from assigning bracing to curves we know will be easily treated. The end result of this ground breaking study was that bracing was successful 72% of the time compared to 48% when nothing was done at all 29. We’ve mentioned before that this study was ended early because it was deemed unethical to continue randomly assigning kids to a “do nothing” ground when bracing was found to be effective. Considering ~60% of participants rejected the idea of being randomized to begin with, you can see the difficultly in performing this kind of solidly objective research. However, it is these types of studies that provide the best evidence supporting the effectiveness of bracing.
Objective scientific research proves scoliosis bracing to be effective
There also have been some great long-term studies that looked to see whether bracing results last a lifetime. In addition to the long term studies we have already mentioned that followed patients for 20 years and found no progression, recent studies have found that reducing a curve is long lasting as well. Between the Mehta study which took advantage of the adolescent growth spurt to straighten the spine by adulthood 30, to the 2017 study that found a >10º reduction could be held for 15+ years 31, we discover once again that research finds bracing for scoliosis is effective, and that early intervention with bracing and physiotherapy 32 can prevent surgery and progression, while reducing curves 33.
Closing Remarks
It can be difficult to find reliable medical information on scoliosis bracing, especially when the research spans so many years and has evolved so much over time. Science and medical research is hard to understand and predatory doctors and clinics know this. The best misinformation is a shred of truth wrapped up in a bunch of nonsense while appealing to your emotions and this is precisely what these groups do.
What everyone SHOULD do is explain all of the research, acknowledge the short comings of some studies, emphasize the good research, and show the big picture and summary so patients and parents can be well informed. Instead, some prey upon things people don’t understand, highlight a few old studies, and slap a “it doesn’t work” label on it and make you believe them simply because someone has a Dr. in front of their name. While a skeletally mature adult with a 50º may not see much improvement with a brace, for a growing child bracing can mean the difference between a smaller curve or surgery. So the take home message is: bracing is effective at treating scoliosis when done correctly. If you would like to read more about scoliosis treatment, we have a page dedicated to discussion various aspects of a successful treatment program. You can also find another fact check article that discusses the question of how long results last once the brace comes off in more detail.
Catch a curve early, treat it early, and treat it according to what research has shown, and whether bracing will work or not is no longer the question. Now the question becomes just how straight can we make that spine.
The recipe for bracing success is simple: Treat a scoliosis as early as possible; straighten the spine as much as possible in-brace; wear the brace as close to 24 hours a day as possible; wear the brace until skeletal maturity; and slowly wean off the brace.
References
- Danielsson, A. J. & Nachemson, A. L. Radiologic findings and curve progression 22 years after treatment for adolescent idiopathic scoliosis. Comparison of brace and surgical treatment with matching control group of straight individuals. Spine 26, 516–525; 10.1097/00007632-200103010-00015 (2001).
- Emans, J. B., Kaelin, A., Bancel, P., Hall, J. E. & Miller, M. E. The Boston bracing system for idiopathic scoliosis. Follow-up results in 295 patients. Spine 11, 792–801; 10.1097/00007632-198610000-00009 (1986).
- Price, C. T., Scott, D. S., Reed, F. R., Sproul, J. T. & Riddick, M. F. Nighttime bracing for adolescent idiopathic scoliosis with the Charleston Bending Brace. Long-term follow-up. Journal of pediatric orthopedics 17, 703–707 (1997).
- Allington, N. J. & Bowen, J. R. Adolescent idiopathic scoliosis. Treatment with the Wilmington brace. A comparison of full-time and part-time use. The Journal of bone and joint surgery. American volume 78, 1056–1062 (1996).
- Fernandez-Feliberti, R., Flynn, J., Ramirez, N., Trautmann, M. & Alegria, M. Effectiveness of TLSO bracing in the conservative treatment of idiopathic scoliosis. Journal of pediatric orthopedics 15, 176–181 (1995).
- Nachemson, A. L. & Peterson, L. E. Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis. A prospective, controlled study based on data from the Brace Study of the Scoliosis Research Society. The Journal of bone and joint surgery. American volume 77, 815–822 (1995).
- Rowe DE. The Scoliosis Research Society Brace Manual (Scoliosis Research Society, Milwaukee, WI, 1998).
- Rowe, D. E. et al. A meta-analysis of the efficacy of non-operative treatments for idiopathic scoliosis. The Journal of bone and joint surgery. American volume 79, 664–674; 10.2106/00004623-199705000-00005 (1997).
- Castro, F. P. Adolescent idiopathic scoliosis, bracing, and the Hueter-Volkmann principle. The spine journal : official journal of the North American Spine Society 3, 180–185 (2003).
- Katz, D. E. & Durrani, A. A. Factors that influence outcome in bracing large curves in patients with adolescent idiopathic scoliosis. Spine 26, 2354–2361; 10.1097/00007632-200111010-00012 (2001).
- Landauer, F., Wimmer, C. & Behensky, H. Estimating the final outcome of brace treatment for idiopathic thoracic scoliosis at 6-month follow-up. Pediatric rehabilitation 6, 201–207; 10.1080/13638490310001636817 (2003).
- Weiss, H.-R. & Rigo, M. Expert-driven Chêneau applications. Description and in-brace corrections. Physiotherapy theory and practice 27, 61–67; 10.3109/09593985.2010.503991 (2011).
- Kuroki, H. et al. Efficacy of the Osaka Medical College (OMC) brace in the treatment of adolescent idiopathic scoliosis following Scoliosis Research Society brace studies criteria. Scoliosis 10, 12; 10.1186/s13013-015-0036-9 (2015).
- Clin, J., Aubin, C.-É., Sangole, A., Labelle, H. & Parent, S. Correlation between immediate in-brace correction and biomechanical effectiveness of brace treatment in adolescent idiopathic scoliosis. Spine 35, 1706–1713; 10.1097/BRS.0b013e3181cb46f6 (2010).
- Thompson, R. M., Hubbard, E. W., Jo, C.-H., Virostek, D. & Karol, L. A. Brace Success Is Related to Curve Type in Patients with Adolescent Idiopathic Scoliosis. The Journal of bone and joint surgery. American volume 99, 923–928; 10.2106/JBJS.16.01050 (2017).
- Simony, A., Hansen, E. J., Carreon, L. Y., Christensen, S. B. & Andersen, M. O. Health-related quality-of-life in adolescent idiopathic scoliosis patients 25 years after treatment. Scoliosis 10, 22; 10.1186/s13013-015-0045-8 (2015).
- Zaina, F. et al. Bracing for scoliosis in 2014. State of the art. European journal of physical and rehabilitation medicine 50, 93–110 (2014).
- Lusini, M., Donzelli, S., Minnella, S., Zaina, F. & Negrini, S. Brace treatment is effective in idiopathic scoliosis over 45°. An observational prospective cohort controlled study. The spine journal : official journal of the North American Spine Society 14, 1951–1956; 10.1016/j.spinee.2013.11.040 (2014).
- Weiss, H.-R., Tournavitis, N., Seibel, S. & Kleban, A. A Prospective Cohort Study of AIS Patients with 40° and More Treated with a Gensingen Brace (GBW). Preliminary Results. The open orthopaedics journal 11, 1558–1567; 10.2174/1874325001711011558 (2017).
- Hawary, R. E. et al. Brace treatment in adolescent idiopathic scoliosis. Risk factors for failure-a literature review. The spine journal : official journal of the North American Spine Society; 10.1016/j.spinee.2019.07.008 (2019).
- Negrini, S. et al. Braces for idiopathic scoliosis in adolescents. The Cochrane database of systematic reviews, CD006850; 10.1002/14651858.CD006850.pub3 (2015).
- Bernard, J.-C. et al. Evaluation du résultat d’un corset monocoque carbone respectant la respiration (CMCR) dans la scoliose idiopathique chez l’enfant et l’adolescent. Étude rétrospective sur 115 patients. Annales de readaptation et de medecine physique : revue scientifique de la Societe francaise de reeducation fonctionnelle de readaptation et de medecine physique 48, 637–649; 10.1016/j.annrmp.2005.08.004 (2005).
- Negrini, S., Donzelli, S., Lusini, M., Minnella, S. & Zaina, F. The effectiveness of combined bracing and exercise in adolescent idiopathic scoliosis based on SRS and SOSORT criteria. A prospective study. BMC musculoskeletal disorders 15, 263; 10.1186/1471-2474-15-263 (2014).
- Karavidas, N. Bracing In The Treatment Of Adolescent Idiopathic Scoliosis. Evidence To Date. Adolescent health, medicine and therapeutics 10, 153–172; 10.2147/AHMT.S190565 (2019).
- Sanders, J. O. et al. Bracing for idiopathic scoliosis. How many patients require treatment to prevent one surgery? The Journal of bone and joint surgery. American volume 96, 649–653; 10.2106/JBJS.M.00290 (2014).
- Maruyama, T., Kobayashi, Y., Miura, M. & Nakao, Y. Effectiveness of brace treatment for adolescent idiopathic scoliosis. Scoliosis 10, S12; 10.1186/1748-7161-10-S2-S12 (2015).
- Aulisa, A. G. et al. Lyon bracing in adolescent females with thoracic idiopathic scoliosis. A prospective study based on SRS and SOSORT criteria. BMC musculoskeletal disorders 16, 316; 10.1186/s12891-015-0782-0 (2015).
- Zaina, F. et al. Research quality in scoliosis conservative treatment. State of the art. Scoliosis 10, 21; 10.1186/s13013-015-0046-7 (2015).
- Weinstein, S. L., Dolan, L. A., Wright, J. G. & Dobbs, M. B. Effects of bracing in adolescents with idiopathic scoliosis. The New England journal of medicine 369, 1512–1521; 10.1056/NEJMoa1307337 (2013).
- Mehta, M. H. Growth as a corrective force in the early treatment of progressive infantile scoliosis. The Journal of bone and joint surgery. British volume 87, 1237–1247; 10.1302/0301-620X.87B9.16124 (2005).
- Aulisa, A. G. et al. Curve progression after long-term brace treatment in adolescent idiopathic scoliosis. Comparative results between over and under 30 Cobb degrees – SOSORT 2017 award winner. Scoliosis and spinal disorders 12, 36; 10.1186/s13013-017-0142-y (2017).
- Berdishevsky, H. et al. Physiotherapy scoliosis-specific exercises – a comprehensive review of seven major schools. Scoliosis and spinal disorders 11, 20; 10.1186/s13013-016-0076-9 (2016).
- Shakil, H., Iqbal, Z. A. & Al-Ghadir, A. H. Scoliosis. Review of types of curves, etiological theories and conservative treatment. Journal of back and musculoskeletal rehabilitation 27, 111–115; 10.3233/BMR-130438 (2014).