Written and reviewed for scientific and factual accuracy by Dr. Austin Jelcick, PhD and Dr. Matthew Janzen, DC
Scoliosis Brace Problems and How to Fix Them
Bracing has been proven by science to not only prevent surgery, but also help straighten the spine of people with idiopathic scoliosis 1, 4. But how are scoliosis braces made? What does the process involve? Who makes scoliosis braces? Why do some doctors say a brace can’t straighten the spine but only prevent it from getting worse? And why are there so many stories on Facebook and social media where bracing failed and the patient ended up having to have surgery?
The answer boils down to two important issues:
- Mistakes are made during the brace design
- Underlying problems that limit bracing success are not addressed
We will talk about the brace design and fitting process here at Scoliosis Care Centers, as well as how it differs from “standard” bracing. We will also talk about how we take care of those underlying problems so bracing can be as successful as possible.
One thing you will probably notice right away is that there is nothing magical about our braces, the difference is in what we do before, during, and after the brace is made and fit. This is what makes the Silicon Valley Method so different and why we are successful in treating adolescent idiopathic scoliosis.
Making Sure The Brace Can Straighten The Spine
First, before we even begin designing or fitting a brace for scoliosis, we work with the patient to treat contractures that are holding their spine in a “stuck”, curvy and coiled position. You can learn about contractures and how we treat them, but essentially, you can think of contractures as stiff tissue that is holding the spine in that “stuck” position.
If you have ever broken a bone and worn a cast, you know how when the cast comes off, you have to stretch and do physical therapy to get back to your normal range of motion. This is because muscles, ligaments, and connective tissue will stiffen over time when it is not used and held in a particular position. Thus, if we don’t treat contractures, these stiff tissues work against us and prevent straightening the spine as much as possible.
This process of releasing contractures non-surgically takes time, and our patients typically will spend one or two weeks, working every day to tackle the contracture problem before we scan them for their brace.
This is absolutely critical because scientific research has shown that getting the spine as straight as possible in the brace determines treatment success.
By treating contractures, we loosen up the spine, allowing us to move the spine into a more corrective position when we brace!
Scanning Before Making the Brace
After we have loosened up the spine to allow us to get it as straight as possible in a scoliosis brace, we perform a scan of the patient as the first step in the brace design process. One important thing to mention here is that the scan is performed while the patient is lying down or in a supine position. This allows the body to be taken out of gravity, and also allows the doctor or clinician to position them into a corrective and elongated position.
Another benefit to scanning the patient in this supine, corrective position is the scan is taken when they are not in a collapsed, curvy position. Quite frequently a scan, measurement, or casting for a brace is made when the patient is standing and not in a corrective position so their spine is still in a collapsed, curvy position. This is a problem because it limits how corrective the brace can be, which limits how straight the spine is in the brace. Science has shown that how straight the spine is in a brace corresponds to how successful treatment will be; therefore the treatment success is already limited due to a mistake being made at the scanning/measurement stage.
Designing a Corrective Brace for Scoliosis
Once the scan has been taken, the brace is modeled and designed based on the scan. At our clinic, the same doctors that treated their contractures, and have an intimate knowledge of that patient’s curve, spine, personality, and limitations are ALSO designing the brace. This ensures that the brace is designed based on that individual patient and all the knowledge gained from working with them for several weeks.
Quite frequently “off the shelf” braces are used which are not designed based on an individual’s particular curve and spine. Another thing that frequently happens is that the brace is designed remotely as one person takes the scan and then send sit off for the brace to be designed elsewhere, or simply by a different person who hasn’t worked with the patient.
The Process of Fitting the Brace to the Patient
After the scoliosis brace has been modeled and designed, it is manufactured to the exact specifications of the design. Once it is ready, the same doctors that have worked with the patient up until now (scanning, modeling and designing) are also the ones who will fit the brace to the patient. Once again this intimate knowledge of the patient and their spine and particular case of scoliosis is critical to ensuring the brace fits as best as possible.
The fitting process has two main goals, and the first is to maximize how straight the brace makes the spine. The fitting process is not simple, and during this process the brace may be tweaked and adjusted to ensure the spine is as straight as possible. This is once again a huge difference from “off the shelf” braces which are “cookie cutter” and are not customized to patient, reducing how straight the spine can be made and thus how effective treatment is.
The second goal is to make the brace as comfortable as possible. To do this, pads are shaped to contour and fit to the patient’s body while parts of the brace may be trimmed or modified to ensure comfort. Ensuring the brace is comfortable is incredibly important because if the brace is uncomfortable, the patient may wear it less, defeating the purpose of the brace. We know from scientific research that the longer you wear a brace the more successful it is, so ensuring the patient is comfortable and wears the brace is fundamental to their success. However, making the brace comfortable needs to be done carefully so that the integrity of the brace design isn’t compromised, limiting how much it can straighten the spine.
It is also important to understand that many “custom” or “designer” braces which are made for a patient are designed by one person while the fitting is performed by another. In fact, quite often the designer is half way around the world as many types of braces are designed in Europe or other countries. The brace designer has obviously never seen the patient, and designs the brace solely based on the measurements or specifications given to them.
As you can imagine, this creates something like a game of telephone where details can be missed. At the very least, the scoliosis brace isn’t being made with as much attention to detail simply because the designer and the fitter don’t have knowledge of, and experience with the patient. Additionally, since the brace is designed so far away the entire process can take longer and delay treatment. Even worse, small but important details can be missed, resulting in a less effective brace.
As you would imagine both designing a brace and fitting a brace require knowledge and skill. However, the fitter may not be educated in brace design. In fact some fitters are trained over weekend seminars teaching how to fit a brace without any real clinical experience required. Thus when the brace is being fit to the patient, the fitter doesn’t know if the brace is a good or bad design, or something in-between.
They won’t know if the brace could be improved, or if modifications made during fitting may compromise how straight the brace can make the spine. It is for this reason that in our clinic, the same doctors that design the brace also fit the brace. This ensures the brace is as good as it can be, corrects the scoliosis and straightens the spine as much as possible, all while remaining as comfortable as possible for the patient to wear.
Checking the Brace and Making it Better
Finally, after the brace is made and fit to the patient, we will check immediately to see just how good of a job it is doing at straightening the spine. We do this using a standing MRI machine and do this for several important reasons.
First, we utilize standing MRI instead of x-ray so that we eliminate any radiation exposure to the patient. Because we are no longer using x-rays and radiation, we can look at the spine and check the brace as much as we need to so we ensure the brace straightens the spine as much as possible. This simply can’t be done with x-ray because it would expose the patient to too much radiation, and while we know radiation can cause cancer, scientific studies have shown higher cancer risks for scoliosis patients BECAUSE of how often they had to have x-rays 2, 3. Thus, eliminating radiation is a key step to improving patient care.
Second, we utilize STANDING MRI so we can see how the brace corrects the scoliosis while the patient is standing and under the effects of gravity. You are probably familiar with standard MRIs which are like long tubes you lay down in. The problem with these is that we aren’t looking at the spine when it is under gravity. Since we spend most of the day on our feet or sitting under the effects of gravity, we want to make sure the brace works well during normal situations and day to day activities.
Third, we use the MRI to continue to look at the brace and the spine to make sure that at every visit and follow up, the brace is still doing its job and doing the best job possible to straighten the spine. This is completely different than standard bracing care where the brace and spine typically aren’t even looked at until 1 month after the fitting. However, doing this can be dangerous, because the patient goes home with a brace that may not be as corrective as possible, or even worse, the brace could be making the curve worse and causing irreparable harm. Needless to say, waiting any amount of time after fitting the brace to check and see if it is doing its job is just stupid, when it can be checked BEFORE the patient goes home with the brace.
Fixing the Deteriorating Brace Problem
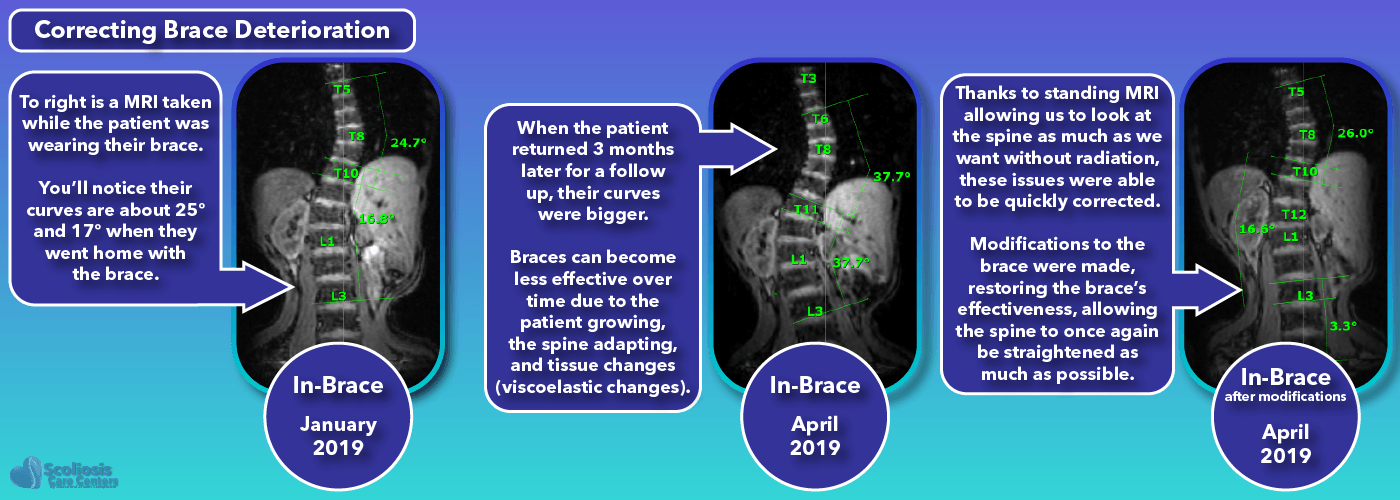
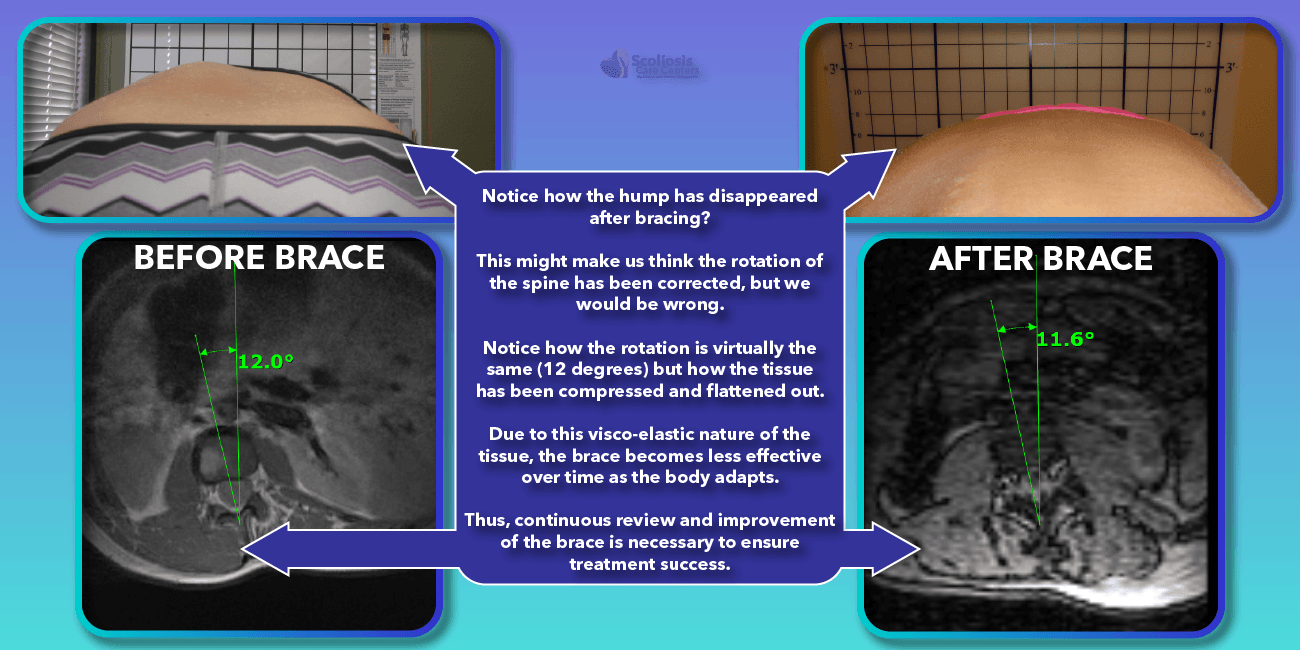
Another important reason to check the brace’s effectiveness at each visit is that the effectiveness of the brace will deteriorate over time. This is something that happens regularly due to the nature of various tissues in the body including fat (adipose tissue), muscle, and connective tissue (ie. Ligaments): the tissues have visco-elastic properties. Visco is short for viscous while elastic is just that, elastic.
How this affects bracing and results in a brace worsening over time can be understood by looking at the pictures below, but the concept is simple. As we apply pressure (from the brace) to the body, the tissues will slowly flatten out, or compress. This creates a problem, because the brace pushes on various parts of the body to push the spine into a straighter position. If our visco-elastic tissues (fat and muscle) begin to flatten out and compress, we lose the contact point where we were pushing. When this happens, we may think the spine is more straight or de-rotated than it actually is because the soft tissue looks like we made a difference, but the spine is no longer being pushed in the right direction because the spot we were pushing on has flattened out, and so we lose that leverage and force.
Additionally, as we progress through bracing treatment, we will slowly change ligaments and connective tissue as well as the spine is straightened more and more. But as it straightens, we once again lose our contact points and the effectiveness of the brace decreases. Therefore, we have to regularly check the brace throughout treatment to make sure it is still doing a good job straightening the spine. If it isn’t then we need to adjust the brace, or perhaps even make an entirely new brace based on the new position of the patients’ body. This ongoing review and revision process is a key ingredient to what makes a bracing treatment as successful as it can be.
After all, we know from scientific research that the formula for bracing success and results that last 20+ years are:
- How straight the brace makes the spine (immediate in-brace correction)
- How long you wear the brace each day (time in brace)
- Treating scoliosis as early as possible (early intervention before structural changes occur)
Eliminating Mistakes Leads to Bracing Success
Current scientific research proved bracing is an effective treatment for idiopathic scoliosis and can not only prevent surgery, but also straighten the spine and provide long lasting results. Yet bracing continues to get a bad rap in part because of misinformation and a lack of knowledge of the current research, but also because mistakes are made during the bracing process that limit how successful the brace can be.
If we eliminate those problems, and improve the entire process with innovations like standing MRI, we can not only be successful with bracing, but make bracing even better than it was before and straighten spines non-surgically.
References
- Aulisa, Angelo G.; Guzzanti, Vincenzo; Falciglia, Francesco; Galli, Marco; Pizzetti, Paolo; Aulisa, Lorenzo (2017): Curve progression after long-term brace treatment in adolescent idiopathic scoliosis. Comparative results between over and under 30 Cobb degrees – SOSORT 2017 award winner. In Scoliosis and spinal disorders 12, p. 36. DOI: 10.1186/s13013-017-0142-y.
- Hoffman, D. A.; Lonstein, J. E.; Morin, M. M.; Visscher, W.; Harris, B. S.; Boice, J. D. (1989): Breast cancer in women with scoliosis exposed to multiple diagnostic x rays. In Journal of the National Cancer Institute 81 (17), pp. 1307–1312.
- Simony, Ane; Hansen, Emil Jesper; Christensen, Steen Bach; Carreon, Leah Y.; Andersen, Mikkel Osterheden (2016): Incidence of cancer in adolescent idiopathic scoliosis patients treated 25 years previously. In European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 25 (10), pp. 3366–3370. DOI: 10.1007/s00586-016-4747-2.
- Weinstein, Stuart L.; Dolan, Lori A.; Wright, James G.; Dobbs, Matthew B. (2013): Effects of bracing in adolescents with idiopathic scoliosis. In The New England journal of medicine 369 (16), pp. 1512–1521. DOI: 10.1056/NEJMoa1307337.